This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
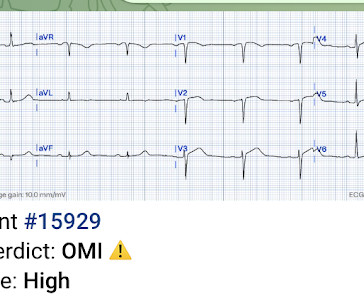
The patient with no prior cardiac history presented in the middle of the night with acute chest pain, and had this ECG recorded during active pain: I did not see any ischemia on this electrocardiogram. The patient has active chest pain, so if these are abnormally large T-waves This link shows 13 blog posts of Posterior Reperfusion T-waves.
Here is his ED ECG: There is bradycardia with a junctional escape. Case continued A bedside ultrasound showed diminished LV EF and of course bradycardia. A 12-lead electrocardiogram, lead V4R , and leads V7-9 were recorded on admission. He appeared gray in color, with cool skin. What is the atrial activity?
The computer interpreted the ECG (GE Marquette 12 SL) as: "Sinus Bradycardia. Here it is: Computer interpretation: "Sinus bradycardia. Comment This paper has received some press recently: Safety of Computer Interpretation of Normal Triage Electrocardiograms The algorithm used was also the GE Marquette 12 SL. Normal ECG."
Smith , d and Muzaffer Değertekin a DIFOCCULT: DIagnostic accuracy oF electrocardiogram for acute coronary OCClUsion resuLTing in myocardial infarction. His first electrocardiogram ( ECG) is given below: --Sinus bradycardia. As he seemed very agitated, fentanyl and diazepam were given.
Here are inferior leads, and aVL, magnified: A closer inspection of the inferior leads and aVL Sinus bradycardia. I had no history on the case and no prior ECG for comparison. What do you think? The T-wave in lead III is slightly tall and broad (increased area under the curve) compared to its QRS complex.
Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias. Figure-1: ECG criteria for diagnosis of a Brugada-1 or Brugada-2 pattern ( See text ). == N OTE : There are numerous additional cases regarding Brugada pattern ECGs by Dr. Smith on this blog ( Simply search for Brugada Syndrome! ).
Regardless of further evaluation, she should avoid bradycardia, AV nodal blockers, Na channel blockers, and fevers. --If Fever not only unmasks a Brugada-type electrocardiogram (ECG) but also increases the risk of ventricular tachyarrhythmias such as ventricular fibrillation (VF) or sudden cardiac death. 8, 2019 ) — ( Jan.
Abnormal Electrocardiogram (ECG): Defined (San Fran syncope rule) as any new changes when compared to the last ECG or presence of non-sinus rhythm. Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful. Abnormal ECG – looks for cardiac syncope.
Theres sinus bradycardia, borderline PR interval, narrow QRS; normal axis/R wave progression; low precordial voltages, and subtle peaked T waves (most obvious in V2, but all T waves are symmetric with a narrow base). Theres no prior ECG to compare - but the bradycardia, prolonged PR and peaked T waves could all be from hyperkalemia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content