This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
KEY Point: Although true that patients with longstanding, severe pulmonary disease may manifest a QRST complex in standard lead I with marked overall reduction in QRST amplitude ( See ECG Blog #65 — regarding Schamroth’s Sign ) — you should never normally see a completely flat line in any of the standard limb leads.
To do this — I apply the P s, Q s, 3 R Approach ( See ECG Blog #185 — for review of my system ). Even if we stopped here — We could conclude the following: There is marked bradycardia in today's rhythm ( ie, Heart rate in the low 30s ). Clinical correlation to sort this all out will clearly be needed. =
By the P s, Q s, 3 R Approach ( See ECG Blog #185 ): The rhythm is fast and QRS complexes are R egular. PEARL # 4: As emphasized in ECG Blog #204 , in which I review derivation of the bundle branch blocks — RBBB is a terminal conduction delay. ECG Blog #185 — Reviews the P s, Q s, 3 R Approach to Rhythm Interpretation.
I see the following: The rhythm is sinus bradycardia at ~55-60/minute. PEARL # 1: As I've emphasized often in this ECG Blog — the course of acute MI from acute coronary occlusion — is often staggered. PEARL # 1: As I've emphasized often in this ECG Blog — the course of acute MI from acute coronary occlusion — is often staggered.
That said — obvious findings include: i ) Marked bradycardia! — Given this patient's older age — if nothing "fixable" is found, she most likely has SSS ( S ick S inus S yndrome ) and will need a pacemaker ( See ECG Blog #342 for more on SSS ). See ECG Blog #188 for review on how to read and/or draw Laddergrams ). be regular! —
It's important to appreciate that we can not rule out the possibility that this rhythm represents Mobitz II 2nd-degree AV block, in which case the patient will need a pacemaker ( See ECG Blog #236 — for review on the ECG diagnosis of the 2nd-degree AV Blocks ). ECG Blog #192 — The 3 Causes of AV Dissociation. STEP-by-STEP.
to 1828 msec. ) — which corresponds to a variation in the rate of sinus bradycardia from 36-to-33/minute. This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute.
NOTE: As I've commented on in a number of previous blog posts — Wenckebach conduction may occur at more than a single level within the AV Node. R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation. ECG Blog #192 — The 3 Causes of AV Dissociation.
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. Smith Pacing in today's case is an effective intervention as doing so prevents the bradycardia and pauses that are likely to precipitate additional episodes of Torsades de Pointes. ( The plan: 1.
See our other countless hyperkalemia cases below: General hyperkalemia cases: A 50s year old man with lightheadedness and bradycardia Patient with Dyspnea. A woman with near-syncope, bradycardia, and hypotension What happens if you do not recognize this ECG instantly? Also: How did this happen? Is this just right bundle branch block?
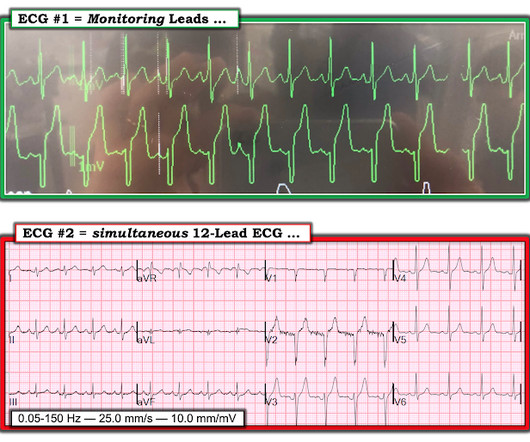
See our other blog posts of hypothermia and Osborn waves -- Massive Osborn Waves of Severe Hypothermia (23.6 Altered Mental Status, Bradycardia == MY Comment , by K EN G RAUER, MD ( 2/2 /2024 ): == Dr. Meyers began today’s case with the clinical challenge of asking you to identify the underlying cause of ECG #2. Is there a long QT?
IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr. Smith's ECG Blog ). Initial high sensitivity troponin I returned at 6ng/L (normal 0.20
Looking first at the long-lead II rhythm strip — there is significant bradycardia , with a heart R ate just under 40/minute. As discussed in ECG Blog #228 — the incidence of " Silent " MI may be as high as between 20-40% of all MIs, being especially common in older individuals. The overall ventricular response looks R egular.
TCP in the ROSC Patient: False Electrical Capture at 75mA Josh Kimbrell, NRP @joshkimbre Judah Kreinbrook, EMT-P @JMedic2JDoc This is the second installment of a blog series showing how transcutaneous pacing (TCP) can be difficult and how you can improve your skills.
Her vital signs were within normal limits except for bradycardia at 55 bpm. It is probably sinus bradycardia with very small/depressed P-waves and prolonged PR interval. P EARL # 4 In my opinion, it is not worth wasting time trying to figure out the specific rhythm diagnosis of a bradycardia when there is hyperkalemia.
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. Smith comment: Go here for a comprehensive blog post on syncope and link to the most detailed version of the Canadian Syncope Rule: Emergency Department Syncope Workup. See these blog posts.
Resuscitation was initiated and this ECG was obtained: Likely AFib (irregularly irregular) with bradycardia. In addition to marked bradycardia — could there be high-grade AV block? On arrival in the ED, she was profoundly hypotensive, nearly obtunded, and bradycardic.
For instance, if there were inappropriate sinus bradycardia at less than 60 bpm, the atrial pacer would take over if it is programmed to wait 1 second before firing. The atrial lead would pace if, after a programmed period of time, it did not sense an atrial beat (usually 1 second, corresponding to a rate of 60).
Both of these features make inferior + RV MI by far the most likely ( Pseudoanteroseptal MI is another name for this ) There is also sinus bradycardia and t he patient is in shock with hypotension. A narrow complex bradycardia without any P-waves is also likely to respond to atropine, as it may be a junctional rhythm.
There was no evidence bradycardia leading up to the runs of PMVT ( as tends to occur with Torsades ). If there had been — a temporary atrial pacemaker could have been considered as a way of increasing the heart rate to suppress a bradycardia-dependent arrhythmia ("overdrive pacing").
The patient has active chest pain, so if these are abnormally large T-waves This link shows 13 blog posts of Posterior Reperfusion T-waves. I did not think that the T-waves in V2 and V3 are hyperacute and I still do not--I disagree with Ken below--I think they are normal , especially in the context of bradycardia.
There’s competing sinus bradycardia and junctional rhythm, with otherwise normal conduction, borderline right axis, normal R wave progression and voltages. Significant bradycardia ( rate in the 40s/minute ) — is present throughout. What do you think? It’s unclear if the paramedic ECGs were seen or missed in the ED.
I will leave more detailed rhythm discussion to the illustrious Dr. Ken Grauer below, but this use of calipers shows that the rhythm interpretation is: Sinus bradycardia with a competing (most likely junctional) rhythm. preceding each of the fascicular beats — indicating a faster rate for the escape rhythm compared to the sinus bradycardia ).
This ECG shows sinus bradycardia with massively long QT (or QU?) Especially when present in the setting of bradycardia and syncopal episodes, this is very worrisome for high risk of lethal dysrhythmias including polymorphic ventricular fibrillation (termed Torsades when in the setting of long QT). interval, at over 600 msec.
This blog explores the ways wearable technology can help track heart health, the advantages it offers, and how it contributes to better outcomes for those requiring surgical intervention. Early detection of conditions like AFib, bradycardia, or tachycardia allows patients to address issues before they become critical.
Josh Kimbrell, NRP @joshkimbre Judah Kreinbrook, EMT-P @JMedic2JDoc This is the first installment of a blog series showing how transcutaneous pacing (TCP) can be difficult, and how you can improve your skills. Learning points: TCP is primarily recommended for bradycardia that does not respond to atropine, or other agents.
My Comment , by K EN G RAUER, MD ( 7/5/2018 ): This blog post provides an excellent example of how a patient with SSS ( = S ick S inus S yndrome ) may present. during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. The indication for pacemaker placement with SSS is symptomatic bradycardia.
Complete Heart Block with Altered Mental Status Josh Kimbrell, NRP @joshkimbre Judah Kreinbrook, EMT-P @JMedic2JDoc This is the third installment of a blog series showing how transcutaneous pacing (TCP) can be difficult and how you can improve your skills. Rhonchi are auscultated bilaterally.
I've copied KEY points from My Comment in the August 6, 2022 post in Dr. Smith's ECG Blog — regarding the answer to this question. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). RBBB in blunt chest trauma seems to be indicative of several RV injury.
Learning points: Your differential for wide QRS (by itself) and bradycardia (by itself) must include hyperkalemia. Labs resulted, showing a potassium of 8.0 mEq/L, glucose of greater than 900 mg/dL, and anion gap metabolic acidosis consistent with DKA. The patient stabilized and was transferred for ICU admission.
He has been following the blog for 4 years. The app also states that there is "suspected" ACS without ST elevation (NSTEMI), posterior fascicular block, sinus bradycardia, and LVH) Note on version 1 of the Queen: she will diagnose "OMI" whether it is an active or reperfused OMI. He wanted to share one of the first cases.
During the night, while on telemetry, the patient became bradycardic, with periods of isorhythmic AV dissociation (nodal escape rhythm alternating with sinus bradycardia), and there were sporadic PVCs. This is what T-waves look like when there is a long QT." Below are two ECGs from the telemetry monitoring.
Syncope and Bradycardia Syncope in a 20-something woman Long QT: Do not trust the computerized QT interval when the QT is long An Alcoholic Patient with Syncope Cardiac Arrest. Is it STEMI? Chest pain in high risk patient. Are these Hyperacute T-waves? What is going on here? What does the ECG show?
Due to bradycardia, a 12-lead ECG was obtained: There is atrial fibrillation at a rate of 54. But because of bradycardia, a 12-lead was obtained, which gave the critical diagnosis. This patient was found with a bottle of alcohol and altered mental status. His breath alcohol was 0.259. The QRS is 166 ms. Why is it slow?
The ECG shows sinus bradycardia but is otherwise normal. Evidence regarding intervention to non-culprit plaques is mixed and beyond the scope of this blog post. We have on many occasions in Dr. Smith's ECG Blog, highlighted the downside of indiscriminate use of morphine in patients who present with new ischemic CP ( C hest P ain ).
The computer called "Sinus Bradycardia" only (implying that everything else is normal. The overreading Cardiologist called it only "Sinus Bradycardia" with no other findings. The rhythm in Figure-1 is sinus bradycardia and arrhythmia. Here is the old ECG from 6 years prior: Notice the inferior T-waves have normal size here.
He suffered from symptomatic bradycardia and falls for over a month and was seen by another cardiologist specifically for presyncope, and still the problem went unrecognized despite ongoing ECG evidence of pacemaker malfunction, and imaging proving lead dislodgement.
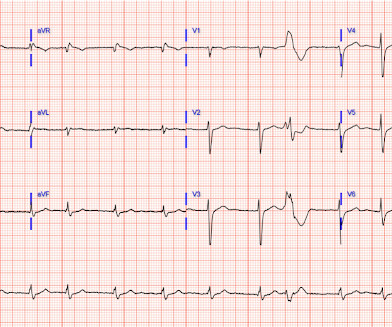
As per Dr. Nossen — today's initial ECG ( LEFT tracing in Figure-2 ) shows sinus bradycardia with QRS widening due to bifascicular block ( RBBB/LAHB ). There is marked, diffuse ST segment depression in ECG #1.
This has been discussed many times before on this blog. In-depth discussion is beyond the scope of this blog. The rhythm is AIVR -- accelerated idioventricular rhythm. There are three mechanisms of arrhythmia: automatic, re-entry, and triggered. Do not treat AIVR. In fact, use of antidyrhythimcs (e.g.,
Three months prior to this presentation, he received a pacemaker for severe bradycardia and syncope due to sinus node dysfunction. Regular readers of Dr. Smith's ECG Blog are well familiar with what is perhaps my favorite Stephen Smith Adage = "You diagnose acute pericarditis at your peril!"
Case continued Another ECG was recorded 3 hours later, still 1/10 pain: There is sinus bradycardia with RBBB. They only mask the underlying pathology. Aspirin and heparin were given, but no NTG. There is minimal STE in I and aVL, but this can be quite normal in RBBB. There is some minimal reciprocal STD in inferior leads.
We've presented numerous examples of hyperkalemia on Dr. Smith's ECG Blog. As a reminder of why determination of the cardiac rhythm can be so challenging when there is significant hyperkalemia — I've reproduced Figure-1 from My Comment in the January 16, 2022 post in Dr. Smith's ECG Blog. WHY Isn't the QRS Wide?
This was a very complex case and the details are too much for an ECG Blog, but suffice it to say that, s hortly thereafter, the patient had an asystolic arrest and was resuscitated. He was placed on ECMO. Peak troponin I at 24 hours was 480 ng/L. Laddergram Illustration: The mechanism of AV block in ECG #2 is complex.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content