This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
And as per ECG Blog #350 — this could represent Wellens ' Syndrome IF this chest lead T wave inversion was new and occurred in a patient who initially had a normal ECG, and then had an episode of transient CP that had resolved at the time this ECG with chest lead T wave inversion was recorded.
As discussed in ECG Blog #231 — Bidirectional VT is a special form of VT, in which there is beat-to-beat alternation of the QRS axis. See My Comment in the June 1, 2020 post in Dr. Smith's ECG Blog — for review of Pleomorphic VT. Multifocal vs Polymorphic VT — September 23, 2011 post from Dr. S.
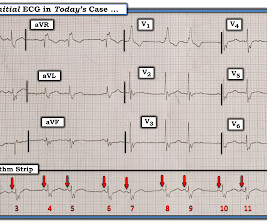
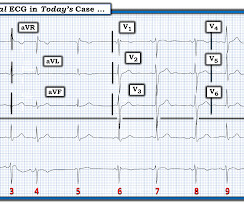
Regarding the 1 2- L ead E CG: Applying the systematic approach I favor for 12-lead ECG interpretation ( as detailed in ECG Blog #205 ): Rate & Rhythm: As stated above — there is a regular, supraventricular rhythm with some P waves, group beating, and an acceptable overall ventricular rate between ~60-80/minute. I begin with Figure-5.
KEY Point: Although true that patients with longstanding, severe pulmonary disease may manifest a QRST complex in standard lead I with marked overall reduction in QRST amplitude ( See ECG Blog #65 — regarding Schamroth’s Sign ) — you should never normally see a completely flat line in any of the standard limb leads.
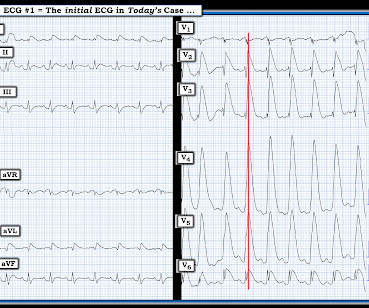
As discussed in ECG Blog #364 and ECG Blog #265 — We are looking at " Shark Fin " ST elevation! Alternatively — the shape of the ST elevation in lead V2 might also be consistent with a component of Brugada Phenocopy ( See ECG Blog #238 ). ECG Blog #265 and ECG Blog #364 — Review cases of Shark-Fin ST Elevation.
For more regarding ECG criteria for LVH — See the ADDENDUM below and/or ECG Blog #73 and ECG Blog #245. A bout H CM ( Different Forms of this Entity ): I've excerpted what appears below from My Comment in the December 26, 2023 post in Dr. Smith's ECG Blog. ECG Blog #245 — Reviews the ECG diagnosis of LVH.
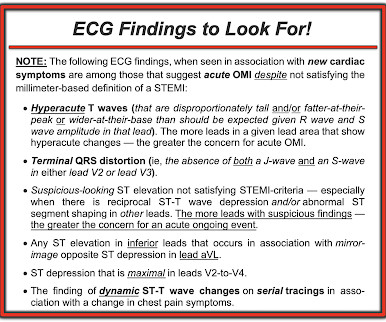
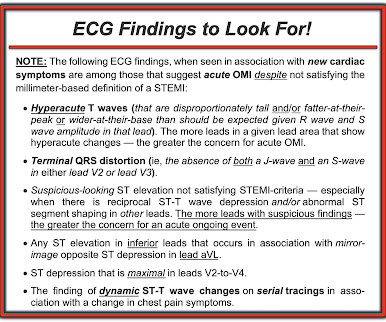
As discussed in many posts in this ECG Blog — despite not satisfying the millimeter-based definition of a STEMI — in this patient with new chest pain, the ECG findings in Figure-1 merit prompt cath lab activation without any need to wait for serum troponin to return elevated ( See ECG Blog #193 — regarding the new "OMI" paradigm ).
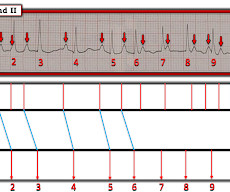
MY Approach to the Rhythm in Figure-1: As per ECG Blog #185 — I favor the P s, Q s, 3 R Approach for interpretation of the cardiac rhythm — beginning with whichever of these 5 KEY Parameters is easiest to assess for the tracing in front of me: At least in the single lead II rhythm strip seen in Figure-1 — The Q RS complex appears to be narrow.
Voltage for LVH is satisfied — at least by Peguero Criteria ( Sum of deepest S in any chest lead + S in V4 ≥23 mm in a woman — as discussed in ECG Blog #73 ). In the October 15, 2022 post of Dr. Smith's ECG Blog — Drs. I've reviewed my approach to the ECG diagnosis of LVH ofte n ( See ECG Blog #245 — among many other posts ).
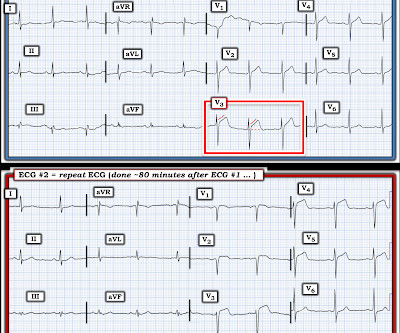
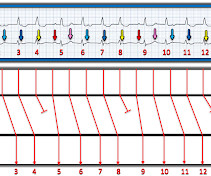
Regarding ST-T Wave Changes in Figure-2: As per the title of today's ECG Blog — one KEY lead "tells the tale". R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation. ECG Blog #294 — Reviews how to tell IF the " culprit " artery has reperfused.
By the P s, Q s & 3 R Approach ( which I review on ECG Blog #185 ): The R ate of the rhythm in Figure-1 is somewhat fast — averaging ~100/minute ( ie, with an R-R interval close to 3 large boxes in duration for most of the tracing ). ECG Blog #229 — reviews distinction between AFlutter vs ATach.
Easy LINKS — tinyurl.com/KG-ECG-Podcasts — [link] — Other ECG Audio PEARLS I previously made for my ECG Blog can be found in the right column of each page on this blog just below this icon — under, "ECG Audio PEARLS". I recently recorded a series of 4 podcasts regarding KEY concepts in ECG interpretation.
MY Approach to the Rhythm in Figure-1: As per ECG Blog #185 — I favor the P s, Q s, 3 R Approach for interpretation of the cardiac rhythm — beginning with whichever of these 5 KEY Parameters is easiest to assess for the tracing in front of me: At least in the single lead II rhythm strip seen in Figure-1 — The Q RS complex appears to be narrow.
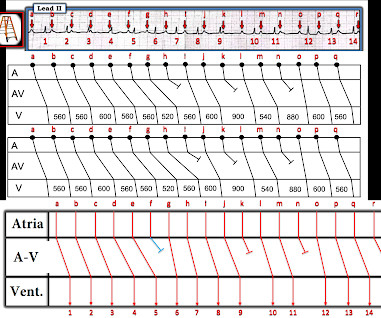
MY Impression of ECG #1: The above 5 Observations confer ECG features that characterize "the Footprints of Wenckebach!" — which is why within seconds of seeing today's ECG, I was virtually certain there was some form of 2nd-degree AV Wenckebach ( See ECG Blog #164 — ECG Blog #55 — ECG Blog #347 — and ECG Blog #154 ).
To EMPHASIZE: One of my goals in developing this ECG Blog — is to help clinicians to optimize their time efficiency. By the P s, Q s, 3 R Approach ( See ECG Blog #185 ) — the rhythm in the long-lead II of Figure-1 is not R egular. That said, as emphasized in ECG Blog #312 — SA block is rare!
By the Ps, Qs, 3R Approach ( which I review in ECG Blog #185 ): P waves are present — and best seen in lead V1. As discussed in detail in ECG Blog #192 — there are 3 Causes of AV Dissociation: i ) By "default"; ii ) By "usurpation"; and , iii ) As a result of AV block. ECG Blog #192 — The 3 Causes of AV Dissociation.
For additional examples of this phenomenon whereby automatic truncation of an EMS ECG may mistakenly result in LVH serving to mimi c ischemia — Check out My Comment at the bottom of the page of the following posts in Dr. Smith's ECG Blog — the November 29, 2023 post — June 20, 2020 — March 31, 2019 — March 29, 2019 — and t he December 27, 2018 post.
PEARL # 1: Although seeing an elevated Troponin would provide additional support for immediate cardiac catheterization — the clinical reality is that the initial Troponin reading will not always be elevated in patients with acute coronary occlusion ( See March 24, 2023 post in Dr. Smith's ECG Blog ).
As reviewed in ECG Blog #350 — t he clinical significance of Wellens' Syndrome — is that its recognition tells you that the patient has a high-grade LAD narrowing with presumably "hot" thrombus h avin g high propensity to propagate and/or totally occlude the LAD at any point in time ( including immediately ). What is W ellens’ S yndrome ?
It's important to appreciate that we can not rule out the possibility that this rhythm represents Mobitz II 2nd-degree AV block, in which case the patient will need a pacemaker ( See ECG Blog #236 — for review on the ECG diagnosis of the 2nd-degree AV Blocks ). ECG Blog #192 — The 3 Causes of AV Dissociation. STEP-by-STEP.
NOTE: As I've commented on in a number of previous blog posts — Wenckebach conduction may occur at more than a single level within the AV Node. R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation. ECG Blog #192 — The 3 Causes of AV Dissociation.
Based on ECG Blog #351 ( www.tinyurl.com/KG-Blog-351 ) LINK to this Page — www. tinyurl.com/KG-MedAll-351 — = = ECG Blog #205 = The Systematic Approach I favor. The "formula" = [link] LINK for Blog #205 = [link] - = Figure: The Systematic Approach that I favor. The talk will be recorded and posted on-line.
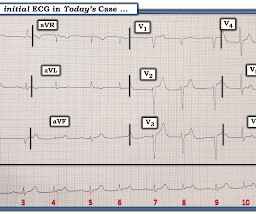
== P lease N OTE : After today — No new ECG Blog posts for 2- to -3 weeks. — I will also not be prompt in replying to emails. == All material on this ECG Blog site remains open! IF you scroll down a little on the right-hand column of this blog — You'll see a lot of icons. Figure-1: The initial ECG in today's case.
Although this " Imbalance " of precordial T waves is not see n very often — in the “right” clinical setting, it has been associated with recent OMI ( O cclusion-based MI ) , most often from a LCx culprit artery ( See Manno et al: JACC 1:1213, 1983 — and the July 17, 2013 post by Salim Rezaie in ALiEM — and ECG Blog #350 ).
. = = R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation. ECG Blog #185 — Review of the P s, Q s, 3 R Approach for systematic rhythm interpretation. ECG Blog #271 — Reviews the concept of diffuse Subendocardial Ischemia. ECG Blog #316 — The patient died.
By the P s , Q s , 3 R Approach ( See ECG Blog #185 ): The rhythm in Figure-1 is clearly not R egular. PEARL #2: As cited in ECG Blog #252 — my favorite truism in arrhythmia interpretation is, "The commonest cause of a pause is a blocked PAC". ECG Blog #185 — Review of the P s, Q s, 3 R Approach for systematic rhythm interpretation.
As always — I like to start by focusing on the long lead rhythm strip — which shows a bigeminal rhythm — in that there are repetitive 2-beat groups ( See ECG Blog #232 for review of the concept of “bigeminy” ). PEARL # 1: As discussed in ECG Blog #232 — it helps to consider the differential diagnosis of a bigeminal rhythm.
In Figure-1 is the ECG from the August 26, 2009 post in Dr. Smith's ECG Blog ( this being one of the 10 Cases of Inferior HATWs that Dr. Smith links to — and the ECG for which he gives a preview of the HATW model that he and Dr. Meyers are working on ). Figure-1: ECG from the August 26, 2009 post in Dr. Smith's ECG Blog.
By the P s, Q s, 3 R Approach ( as reviewed in ECG Blog #185 ): The Q RS complex is obviously wide. R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation. ECG Blog #185 — Systematic P s, Q s, 3 R Approach to Rhythm Interpretation. I do not see P waves.
Although this " Imbalance " of precordial T waves is not seen very often — in the “right” clinical setting, it has been associated with recent OMI ( O cclusion-based MI ) from a LCx culprit artery ( See Manno et al: JACC 1:1213, 1983 — and the July 17, 2013 post by Salim Rezaie in ALiEM — and ECG Blog #350 ).
For more on Torsades de Pointes vs PMVT See My Comment in the October 18, 2023 post and the September 2, 2024 post in Dr. Smith's ECG Blog ). Figure-1: My "correction factor" for QTc estimation when the QRS is not wide ( from My Comment in the March 19, 2019 post in Dr. Smith's ECG Blog ).
In this ECG Cases blog, Jesse McLaren and Rajiv Thavanathan explore how ECG and POCUS complement each other for patients presenting to the emergency department with shortness of breath or chest pain. They explain complementary diagnostic insights into pericardial effusion and cardiac tamponade, occlusion MI and RV strain.
In this ECG Cases blog we look at 5 cases of ECGs falsely labeled 'normal'. Can you spot the critical abnormality? Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman. October 2024 Five patients presented with ECGs labeled ‘normal’. Can you use systematic ECG interpretation to identify the [.]
In this ECG Cases blog Dr. Jesse MacLaren guides us through 10 cases of patients who present with generalized weakness or acute neurologic symptoms and discusses how to look for ECG signs of dysrhythmias, electrolyte emergencies, acute coronary occlusion, and demand ischemia in patients with generalized weakness and in patients with neurologic symptoms, (..)
More cases can be found on the blog here. Since then ( as we have shown on already many cases of Dr. Smith's ECG Blog ) — this is actually a surprisingly common phenomenon that all-too-often goes unrecognized ( as per the unnecessary cardiac catheterization that was done in today's case ). "Look how bizarre it is."
In this month's ECG Cases blog Dr. Jesse McLaren reviews interpretation of the pre-arrest ECG: identifying high risk ECGs requiring empiric treatment like calcium for hyperkalemia, magnesium for long QT, or reperfusion for Occlusion MI; the intra-arrest ECG: identifying pseudo-PEA; and post-arrest ECG: the importance of serial ECGs to reduce false (..)
An undergraduate (not yet in medical school) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly arrived at work and happened to glance down and see this previously recorded ECG on a table in the ED. It was recorded at 0530: What do you think?
IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr. Smith's ECG Blog ).
Watch Zeke and Zanes story *This blog post is sponsored by the Heart Institute at Childrens Hospital Colorado. With every act of kindness and generosity, Childrens Colorado isnt just changing lives, says Kayla, its shaping a future in which my boys can be kids and grow up to pursue their dreams.
Each section includes: A brief check list of the OMI ECG criteria Several ECG examples curated from Dr. Smith's ECG Blog The specificity of each criteria with links to relevant literature ? Mark Hellerman — for his excellent work in producing the OMI Pocket Guide , that is the subject of today’s post on Dr. Smith’s ECG Blog.
In this Waiting to Be Seen blog Dr. Howard Ovens outlines 4 key learnings from his extensive career in EM leadership: Be a good clinician, get substantial real-world experience, take a long-term view of benefits and risks and get along with your counterparts in the leadership dyad.
Date Nov 7, 2024 Image Blog Giving Credit Matters. Image Blog Managing Relationships with Patients Early career cardiothoracic surgeons have many important relationships that need to be managed and developed. Here's How to Do It.
In this ECG Cases blog Dr. Jesse McLaren guides us through 10 cases, driving home the points that sepsis is a common cause of rapid Afib and diffuse ST depression with reciprocal ST elevation in aVR, myo/pericarditis is a diagnosis of exclusion, endocarditis or lyme carditis can cause AV block, PE can cause low grade fever and ECG signs of acute RV (..)
Smith comment: Go here for a comprehensive blog post on syncope and link to the most detailed version of the Canadian Syncope Rule: Emergency Department Syncope Workup. See these blog posts. EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content