This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
Background:Little is known about the clinical relevance of interleukin (IL)-6 and the severity of patients with acute ST-elevation myocardial infarction (STEMI). This study examined the possible associations of plasma IL-6 concentrations with TIMI scores in STEMI patients treated with primary percutaneous coronary intervention (PCI).Methods:The
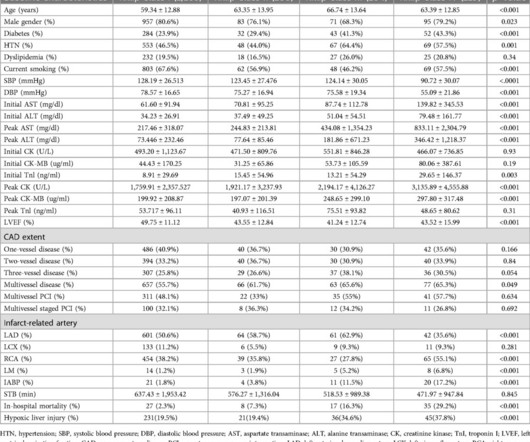
Methods and Results Patients with confirmed ST elevation myocardial infarction (STEMI) treated by emergency medical services were included in this retrospective cohort analysis of the AVOID study. Greater severity of chest pain is presumed to be associated with a stronger likelihood of a true positive STEMI diagnosis. years old ± 13.7
Neural and electrical remodeling are well documented in the acute setting of myocardial infarction (MI). Sympathetic nerve sprouting in the infarct border zone increases transmural dispersion of repolarization, promoting arrhythmias.
IntroductionHypoxic liver injury (HLI) and Killip classification are poor prognostic factors in patients with ST-segment elevation myocardial infarction (STEMI). Both initial and peak AST levels increased in accordance with Killip classification along with cardiac biomarkers.
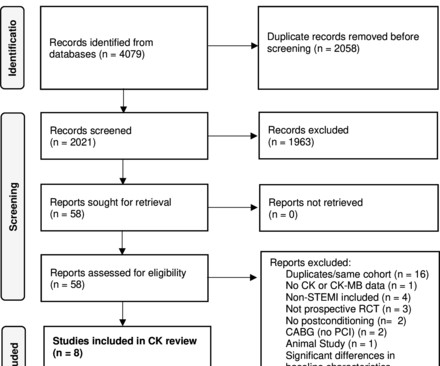
Objectives This study aimed to perform a meta-analysis of the short-term impact of ischaemic postconditioning (IPoC) on myocardial injury in ST elevation myocardial infarction (STEMI) using surrogate cardiac biomarkers. Conclusions IPoC does not seem to protect against myocardial injury in STEMI, except possibly in smokers.
Aim Acute injury and subsequent remodelling responses to ST-segment elevation myocardial infarction (STEMI) are major determinants of clinical outcome. Current imaging and plasma biomarkers provide delayed readouts of myocardial injury and recovery. A total of 72 patients undergoing PPCI for acute STEMI underwent miR analysis and cMRI.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." The ESC states that patients with suspected ACS should go to the cath lab in <2 hours "regardless of ECG or biomarker evidence of MI!!"
This study investigates the relationship between baseline 5-HTP levels and the incidence of major adverse cardiovascular events (MACE) in patients who have experienced ST-elevation myocardial infarction (STEMI).Objective:Our Conclusion:Higher 5-HTP levels are independently associated with a reduced risk of MACE in patients after STEMI.
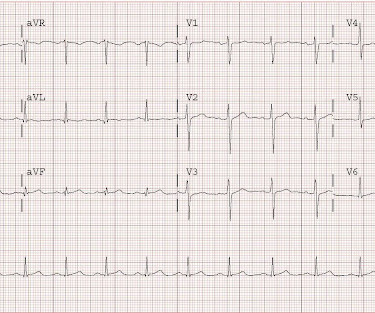
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
By definition, this is a non-STEMI because there is not 1 mm of ST elevation in 2 consecutive leads. Even though the patient's ECG did not meet criteria for STEMI, he had all the pathology of a STEMI. Even though the patient's ECG did not meet criteria for STEMI, he had all the pathology of a STEMI.
His ECG was repeated at this point: This shows a well developed anterior STEMI. To not see these findings is very common, and this patient would be given the diagnosis of NonSTEMI, with subsequent development of STEMI. It is not a missed STEMI, but it is a missed coronary occlusion. The peak troponin I was over 100.
Frick -- one wonders about the diagnosis of unstable angina in a patient with significantly elevated biomarkers which would certainly have been rising on repeat measurement.) The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Is there STEMI? What is the rhythm? Moffat, M.
The ESC states that patients with suspected ACS should go to the cath lab in <2 hours "regardless of ECG or biomarker evidence of MI!!" Comment : ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). Therefore, we activate the Cath Lab.
Considering their multidirectional effect on atherosclerosis, new inflammatory biomarkers integrating various leukocyte subgroups have been proposed to calculate the systemic inflammatory response index (SIRI) and systemic inflammatory index (SII).Aim:The The mean age of patients was 57.68 (SD= 11.19) years.
The "criteria" for posterior STEMI are 0.5 Is it STEMI or NonSTEMI? It was opened and stented with a door to balloon time of about 120 minutes (this is long for STEMI, but very short for a high risk Non STEMI). The troponin I returned at 4.1 ng/mL (ULN = 0.030 ng/mL) , diagnostic of myocardial injury. mm STE in one lead.
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI. Limkakeng AT.
The ECG progression, clinical picture, and biomarkers are also involved in the full diagnosis of OMI. This one likely does meet STEMI criteria in II, III, and aVF. The development of an inferior-posterior STEMI, from prehospital to hospital Inferior hyperacute T-waves. Criteria for a STEMI are definitely not met in ECG #1.
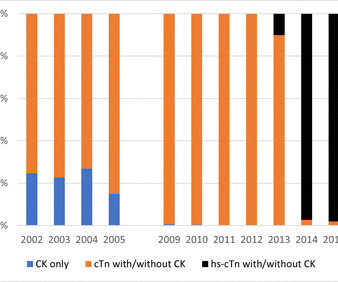
Using person-linked hospitalisation data, we compared International Classification of Diseases (ICD)-coded data with biomarker-classified admission rates for ST-segment elevation MI (STEMI), non-STEMI (NSTEMI) and unstable angina (UA) in Western Australia (WA). Results There were 37 272 ACS admissions in 30 683 patients (64.2%
In acute STEMI, the T-wave is large, whereas in LV aneurysm , the T-wave is not so large. If greater than or equal to 0.22 , then acute anterior STEMI. correlates with anterior STEMI) Rule 2. If there is any one lead of V1-V4 with a T/QRS ratio greater than 0.36, then it is likely to be anterior STEMI. Answer below.
The fear comes built in with the diagnosis often amplified by young felllows on call (& often times by senior consultants as well) It may appear real, from a clinical angle, but trust, when we deal with the whole gamut of so-called ACS (other than STEMI), there is indeed a benign face in many of them.
50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). This correlates with potentially salvageable myocardium. See Raitt et al.: These findings together are more commonly seen with pericarditis.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content