This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
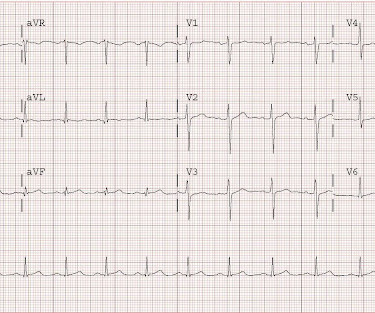
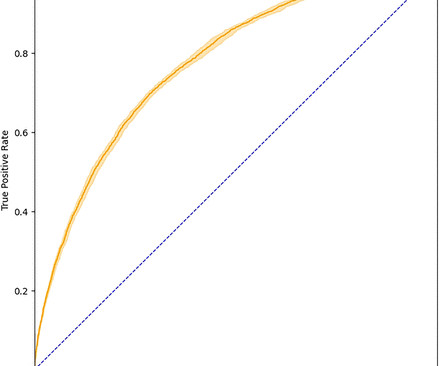
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
This results in severe chestpain or discomfort, with the subsequent release of cardiac biomarkers, and alterations in the electrocardiogram. It can cause diminished heart function and mortality if not treated properly with suitable measures.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. These diagnoses were not found in his medical records nor even a baseline ECG.
Acute pericarditis (AP) is the second most common cardiac cause of chestpain, diagnosed when at least two of the following criteria are met: characteristic pleuritic chestpain, pericardial rub on auscultation, new typical ECG changes (such as widespread ST-elevation or PR-depression) and pericardial effusion on imaging.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. It was not relieved by anything. He had no previous medical history. This includes: 1.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. Triage ECG: What do you think? This is diagnostic of proximal LAD occlusion. This is a huge anterolateral OMI. I cannot be anything else.
Introduction:Over 6 million patients (pts) present to US emergency departments annually with chestpain (CP), of which the majority are found to have no serious disease. Evaluation of these pts results in substantial costs for unnecessary hospitalization and extensive testing.
1 However, with the introduction of high-sensitivity (hs) assays for cTn and the need for biomarkers for cardiovascular risk stratification, their use has expanded beyond the diagnosis of ACS. Cardiac troponin (cTn) plays a key role in diagnosing acute coronary syndrome (ACS) in the emergency department (ED).
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. 1] European guidelines add "regardless of biomarkers". But only 6.4%
See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG. This is different from nitroglycerin which produces vasodilation and can improve by pain improving myocardial perfusion. You do not need to be better than the Queen of Hearts at EKG to understand that refractory chestpain NEEDS CATH NOW.
The patient with no prior cardiac history presented in the middle of the night with acute chestpain, and had this ECG recorded during active pain: I did not see any ischemia on this electrocardiogram. This is a case I had quite a while back. See the explainability : She sees large T-waves in V2, V3.
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. Thanks for reading Dr. The data is overwhelming every way you can possibly look at it.
One study revealed that a quarter of all ED visitors underwent a troponin test, even though less than half of them had chestpain. Another study showed that roughly one in seven ED patients had elevated troponin, even though they weren’t experiencing an MI, in part because troponin can be a sign of other non-coronary diseases.
Additionally, 2D transthoracic echocardiography (TTE), and myocardial injury serum biomarkers assays (creatine phosphokinase-MB [CPK-MB] and cardiac troponins [cTn]) were measured once. Cardiovascular consultation had been requested for all of the patients based on their primary clinical examination, vital signs, and electrocardiogram (ECG).
She did not report any chestpain or pressure. She was brought to the Emergency Department and this ECG was recorded while she was still feeling nauseous but denied chestpain, shortness of breath, or other symptoms: What do you think? A male in his 60s with chestpain A Male in his 60s with Chestpain.
This was my thought: if this patient presented to the ED with chestpain, then this is an LAD occlusion. These patients have worse outcomes: higher mortality, more CHF, higher biomarkers, and worse ejection fractions than the NonSTEMI patients with open arteries. This patient had continued and ongoing pain.
The diagnosis was made based on classic findings of inflammation on an electrocardiogram associated with acute chestpain. 2-3 days after this he developed the same sharp chestpain and shortness of breath with elevated inflammatory markers (CRP) as well as typical findings of pericarditis seen on ECG.
Cardiac Cath labs waiting for some major influx of COVID heart damage not only didn’t see patients presenting with COVID heart attacks, but they idled as patients terrified of coming to the hospital stayed home rather than come to the hospital with chestpain. You could ignore the c19-myo without the conclusions changing much.
Case 2 A 38 year old male with h/o smoking only c/o a few hours of severe substernal chestpain; he thinks he is having a heart attack. The pain is very nitroglycerine responsive. The first ECG with pain (unavailable) showed T wave flattening in V2 and V3. Fortunately, his MI was not large by biomarkers.
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chestpain.
Background Elevated troponin levels are a sensitive biomarker for cardiac injury. The quick and reliable prediction of troponin elevation for patients with chestpain from readily available ECGs may pose a valuable time-saving diagnostic tool during decision-making concerning this patient population.
He presented with chestpain of 48 hours duration which became worse in the previous several hours. The pain was stabbing and 10/10 and associated with SOB. The pain was partly relieved with sublingual nitroglycerin. This patient had no significant past medical history.
Scenario 1 : The patient presents with 24 hours of substernal chestpain. Both reperfusion, as judged by the biomarker curve, and patency, as assessed by the angiogram, were correlated with the rapidity and depth of T wave inversion. He presented to the emergency department for evaluation. Below is his presentation ECG.
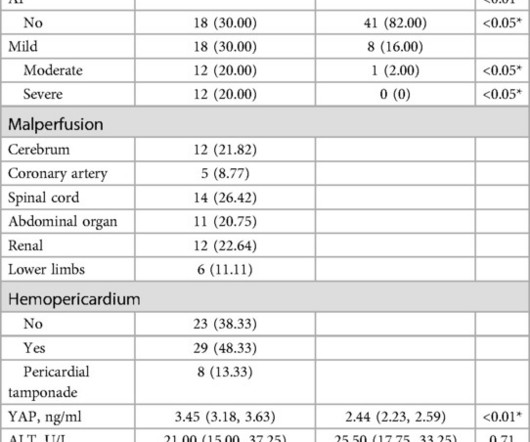
Novel serum biomarkers can potentially help in early detection and estimation of postoperative outcomes. BackgroundAcute aortic dissection is a lethal cardiovascular emergency; early diagnosis is critically necessary. ResultsYAP concentration was substantially elevated among ATAAD patients [3.45 (3.18, 3.63) vs. 2.44 (2.23, 2.59), P<0.01].
How can biomarkers help us grade these ACSs? I don’t understand how the curve of non-cardiac chestpain trespasses in the middle of a Troponin race (False positives? It is next to foolishness to rush them to cath lab. See how the Kaplans diverge dramatically depending upon the hsTnT levels.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content