This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
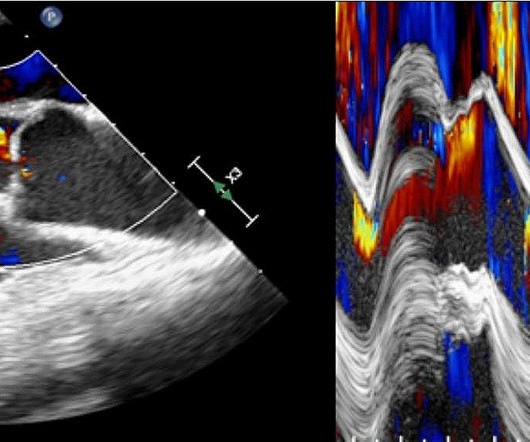
Intra-cardiac thrombosis is a potentially devastating complication of extracorporeal membrane oxygenation (ECMO) mechanical circulatory support. We present here a patient who suffered complete thrombosis of a.
A 76-year-old woman with a history of double valve replacement (Aortic and mitral valves) for rheumatic heart disease, presented with acute dyspnea after a switch from Warfarin to LMWH before a planned bone marrow biopsy. The investigations revealed a stuck aortic prosthetic valve ,that showed a prohibitive gradient of more than 50 mmhg.
Patients with aortic/mitral/tricuspid valve disease or root/ascending aorta >40 mm were included as soon as they were diagnosed with heart valve disease.
Blunt cardiac injury my result in : 1) Acute myocardial rupture with tamponade 2) Valve rupture (tricuspid, aortic, mitral) 3) Coronary thrombosis or dissection (and thus Acute MI) from direct coronary blunt injury 4) Dysrhythmias of all kinds.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. elevated BP), but rather directly correlated with coronary obstruction (due to plaque rupture and thrombosis) and, potentially, stymied TIMI flow. This results in Type I MI.
Additional architectural changes include systolic anterior motion of the mitral valve, endothelial dysfunction at the level of the coronary arterial bed, and ventricular diastolic dysfunction. References Naidu, S. Diagnosis and management of hypertrophic cardiomyopathy: Expert analysis. American College of Cardiology.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










Let's personalize your content