This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
At 30-day follow-up, all-cause mortality, the incidence of major adverse cardiovascular events, major vascular complications, and new permanent pacemaker implantation were 3.8%, 4.6%, 0.8%, and 0.8%, respectively. of patients showedmild paravalvular leakage, and all 125 (100%) patients were in New York Heart Association ClassII.
Food and Drug Administration ( FDA ) confirmed 13 to 1, with 0 abstention that the benefits of Abbott's TriClip™ transcatheter edge-to-edge repair (TEER) system outweighed the risks for the treatment of people with tricuspid regurgitation (TR). On the final question of the benefit of TriClip versus the risk, the vote was 13 to 1 in favor.
BACKGROUND:Data concerning the outcomes of transcatheter aortic valve replacement in type 0 bicuspid aortic stenosis (AS) are scarce. Ascending aortic diameter was the single predictor of 1-year mortality in type 0 bicuspid patients (hazard ratio, 1.59 [95% CI, 1.03–2.44];P=0.035). Poverall=0.522; 1 year: 10% versus 2.3%
BACKGROUND:This study aimed to compare the incidence and prognostic implications of new-onset conduction disturbances after surgical aortic valve replacement (SAVR) in patients with bicuspid aortic valve (BAV) aortic stenosis (AS) versus patients with tricuspid aortic valve (TAV) AS (ie, BAV-AS and TAV-AS, respectively).
Standalone performance for significant major valve disease pathology (aortic stenosis and regurgitation and mitral and tricuspid regurgitation) had a 93 percent sensitivity and 93 percent specificity.
Tricuspid regurgitation (TR): frequency, clinical presentation, management and outcome among patients with severe left-sided valvular heart disease in Europe. ESC-EORP, European Society of Cardiology-EURObservational Research Programme; TV, tricuspid valve.
Patients with bicuspid aortic valves (BAV) are predisposed to the development of aortic stenosis. Single-arm studies, conference presentations, animal studies, and studies that involved patients with tricuspid aortic morphology were excluded. Medical databases were queried to pool comparative studies of interest.
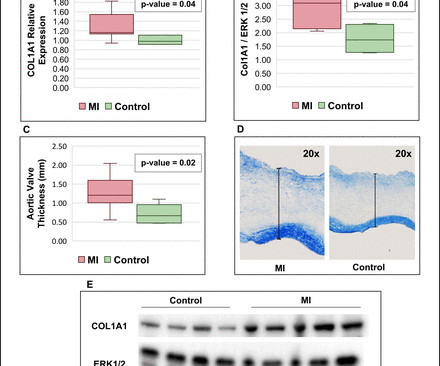
Background Myocardial infarction (MI) has been shown to induce fibrotic remodelling of the mitral and tricuspid valves. It is unknown whether MI also induces pathological remodelling of the aortic valve and alters aortic stenosis (AS) progression.
However, underlying lesions such as hypertension, mitral valve disease, COPD, ASD, and TR greatly influence the degree of atrial enlargement. This is similar to MR begets MR. Atrial functional MR occurs when the lower part of the atria stretches the mitral annulus. No published proof as such.
Much of these SAVR declines occurred in patients with tricuspid aortic valves (from 84.5% to 55% of total SAVRs), while SAVR ratios increased among patients with bicuspid aortic valves (from 15.5% That’s a positive trend given that <80yr SAVR patients with bicuspid aortic valves also had better-than-expected mortality rates.
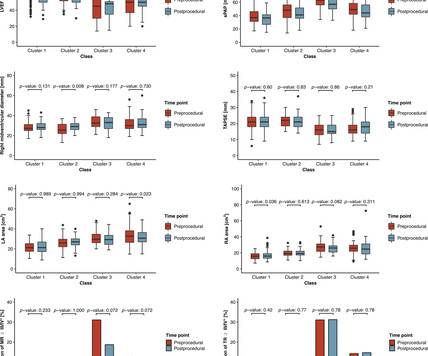
Objective A novel artificial intelligence-based phenotyping approach to stratify patients with severe aortic stenosis (AS) prior to transcatheter aortic valve replacement (TAVR) has been proposed, based on echocardiographic and haemodynamic data. ±15.8 ±15.1 mm Hg, p value: 0.0079).
Proposed approach for clinical management and therapeutic optimization in patients with heart failure with reduced ejection fraction and low blood pressure. Low blood pressure with major or mild symptoms. **SBP SBP <80mmHg or symptomatic low BP or asymptomatic low BP.
Transcatheter valve therapy has evolved from a novel treatment for the sickest patients to become the standard of care for many with aortic stenosis. The rapid adoption of transcatheter mitral and tricuspid therapies has also transformed the treatment landscape, expanding options for patients with structural heart disease.
Transcatheter valve therapy has evolved from a novel treatment for the sickest patients to become the standard of care for many with aortic stenosis. The rapid adoption of transcatheter mitral and tricuspid therapies has also transformed the treatment landscape, expanding options for patients with structural heart disease.
Tracing in the lower part is tissue Doppler imaging from the medial mitral annulus. Opening and closing movements of the aortic and mitral valves are visible. Slight downward angulation of the transducer from this view gives the left ventricular cross section with mitral valve cross section within.
Food and Drug Administration (FDA) approval of its TriClip, a first-of-its-kind device to repair leaky tricuspid heart valve, for which more than 1.6 are affected by tricuspid regurgitation, 1 which can severely impact quality of life. Abbott has announced U.S million people in the U.S. are estimated to be affected. the Roger L.
Objective CT aortic valve calcium score (AVC score ) and density (AVC density ) thresholds have been recommended for aortic stenosis (AS) severity assessment in tricuspid aortic valve (TAV). We aimed to compare AVC score and AVC density in bicuspid aortic valve (BAV) versus TAV.
Background Bicuspid aortic valve (BAV) is often associated with a concomitant aortopathy. This study aimed to compare the progression rate of aorta dimensions according to AV phenotype (BAV vs tricuspid AV (TAV)), fusion type and sex in patients with aortic stenosis (AS).
Adult Cardiac Surgery Database Lead Author Title Publication Date Jacob Raphael Red Blood Cell Transfusion and Pulmonary Complications: The Society of Thoracic Surgeons Adult Cardiac Surgery Database Analysis The Annals of Thoracic Surgery January 2024 Joseph Sabik Multi-Arterial versus Single-Arterial Coronary Surgery: Ten Year Follow-up of One Million (..)
Program Designations Access and Publications (A&P) 1 Participant User File (PUF) 2 Task Force on Funded Research (TFR) 3 Special Projects 4 Adult Cardiac Surgery Database Lead Author Title Publication Date William Keeling 2 National Trends in Emergency Coronary Artery Bypass Grafting European Journal of Cardiothoracic Surgery October 2023 Jake (..)
Objectives Grading the severity of moderate mixed aortic stenosis and regurgitation (MAVD) is challenging and the disease poorly understood. Methods Moderate MAVD was defined as coexisting moderate aortic stenosis (aortic valve area (AVA) 1.0–1.5 –1.5 cm 2 ) and moderate aortic regurgitation (vena contracta (VC) 0.3–0.6
Bernoulli equation (P=4V 2 ) gives the gradient of tricuspid regurgitation flow, which corresponds to the pressure difference between right ventricle and right atrium in systole. If there is high right atrial pressure with elevated jugular venous pressure, 15 or 20 mm Hg may have to be added instead of 10 mm Hg.
AF, atrial fibrillation; LAVI, left atrial volume index; RA, right atrial; RV, right ventricular; sPAP, systolic pulmonary artery pressure; SVI, stroke volume index; TR, tricuspid regurgitation. Aims Paradoxical low-flow, low-gradient aortic stenosis (pLFLG AS) may represent a diagnostic challenge, and its pathophysiology is complex.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content