This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
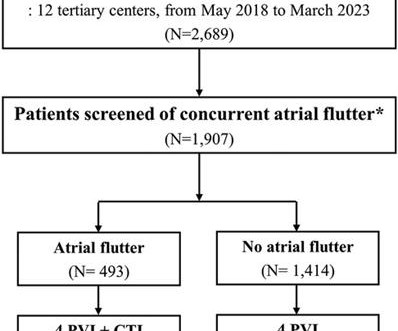
Typical atrialflutter commonly occurs in patients with atrial fibrillation (AF). Limited information exists regarding the effects of concurrent atrialflutter on the long-term outcomes of rhythm control. Patients who were screened for typical atrialflutter were included in the analysis ( n = 1,907).
male with pertinent past medical history including Atrial fibrillation, atrialflutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Description : Regular Wide Complex Tachycardia at a rate of about 160.
Atrialflutter/atrialtachycardia (AFL/AT) detection performance in insertable cardiac monitors (ICM) remains a challenge due to inappropriate detections.
There is a regular narrow complex tachycardia. Thus, it is supraventricular tachycardia. It is important to remember that SVT includes Sinus Tachycardia! Sometimes even Wide Complex Tachycardia is Sinus. See this case in which Lewis leads were necessary to figure this out: Wide Complex Tachycardia.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. The ECG was interpreted as showing atrialflutter with 2:1 conduction. Answer : The ECG above shows a regular wide complex tachycardia. The heart rate could be compatible with that of a 2:1 conducted atrialflutter.
If a wide complex tachycardia occurs, the probability is very high that it is a ventricular tachycardia (approx. Here we see a broad complex tachycardia that looks like an RBBB + LAFB, which is regular. 80%, in patients with a previous myocardial infarction (.) In this constellation, 3 causes must be considered: 1.
Here is his initial rhythm strip (it is not a full 10 seconds): Wide complex tachycardia, rate 235 This is a very wide complex regular tachycardia at a rate of 235. It should be considered to be Ventricular Tachycardia and treated as such. Rate 120, flutter rate 240. Still more ST depression. So what happened?
So it is not atrial fib and not VT. It is a regular narrow complex tachycardia. The fact that the patient is on Flecainide and Diltiazem is good evidence that this is atrialflutter with 1:1 conduction. If you look closely at lead II across the bottom, it appears there are flutter waves. What is the DDx?
Wild-type transthyretin amyloid cardiomyopathy (ATTRwt-CM) is often accompanied by atrial fibrillation (AF), atrialflutter (AFL), and atrialtachycardia (AT), which are difficult to control because beta-blockers and antiarrhythmic drugs can worsen heart failure (HF).
ABSTRACT Atrialflutter (AFL), defined as macro-re-entrant atrialtachycardia, is associated with debilitating symptoms, stroke, heart failure, and increased mortality. Atypical AFL is a heterogenous group of re-entrant atrialtachycardias that most commonly occur in patients with prior heart surgery or catheter ablation.
QUESTIONS: Is this rhythm too fast to be sinus tachycardia? Are flutter waves hidden within the QRS and T waves? However, until such time that we know for certain — I think it best to simply describe what we see: PEARL # 1: Realize that for any tachycardia — there are 6 Parameters that need to be assessed. s in Figure-2 ).
There is a regular wide complex tachycardia. A fully upright P-wave is typical atrial activity of atrialflutter as seen in V1. See these example cases of upright P-waves: Case Continued Thus, I was all but certain that this was atrialflutter. If it is flutter, it will reveal the underlying flutter waves.
Wide-complex tachycardia: VT or aberrant, or "other?" The patient had a history of paroxysmal atrial fibrillation and several cardioversions. A wide-complex tachycardia in an older patient must immediately suggest ventricular tachycardia. Instead, the rate of 150, plus the history of AF, suggested atrialflutter.
Initial ECG in the ED: Presenting ECG : Wide-complex tachycardia at a rate about 200. This is overwhelmingly likely to be ventricular tachycardia, even if only age and medical history are considered. Nevertheless, the widths of both the QRS complex and the RS duration are similar in both the old ECG and the tachycardia.
Primary endpoint was the incidence of patients with new onset supraventricular arrhythmia (AF, atrialflutter or any supraventricular tachycardia) lasting >30s, post PFO closure.ResultsA total of 59 patients met the inclusion criteria.
The positive F wave in lead V1 changed during entrainment from the right atrial appendage (RAA) during typical atrialflutter (AFL). Abstract Introduction Typical atrialflutter (AFL) is a macroreentrant tachycardia in which intracardiac conduction rotates counterclockwise around the tricuspid annulus.
PEARL # 3: At this point — the most time-efficient step for solving today's rhythm will be to determine the nature of atrial activity. C ASE C onclusion : I lack detailed follow-up from today's case — other than knowing that the AtrialTachycardia was controlled. ECG Blog #138 — AFlutter vs AtrialTachycardia.
Let's first consider the heart rate: with a heart rate of 194 beats/min, the heart rate is too low for atrialflutter (1:1) (except in patients who have been pre-treated with medication), and the rate would be unusually high for atrialflutter with 2:1 conduction.
There is the appearance of STE in inferior leads II, III, and aVF (with STD in aVR), but this is entirely due to flutter waves which are only seen in those leads. Also, the atrialflutter in this case is relatively slow like in many other cases we've shown. Tachycardia and ST Elevation. AtrialFlutter with Inferior STEMI?
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? To me, it was clearly atrialflutter with 1:1 conduction. The rate of 280 is just right for atrialflutter. The waves look like atrialflutter waves, NOT like a wide ventricular complex.
The trial will evaluate the outcomes of therapy provided with the FARAPULSE PFA System versus AADs, including device-or procedure-related adverse events, the rates of freedom from AF, atrialflutter, or atrialtachycardia, as well as AF burden – a measurement of the amount of AF an individual experiences.
There is a narrow complex tachycardia at a rate of 130. ECGs: there is a regular narrow complex tachycardia still at a rate of exactly 130, with no P-waves and also no change since the prehospital ECG. Leads II and aVF appear to have flutter waves. I diagnosed atrialflutter with 2:1 conduction. Is is sinus?
When mutiple atrialtachycardias coexist, ablation of an individual isthmus may lead to a seamless transition (without significant changes in surface ECG or coronary sinus activation) to a second rhythm. The isthmus block could go unnoticed leading to continued unnecessary ablations.
Publication date: Available online 17 December 2023 Source: The American Journal of Cardiology Author(s): Hugo De Larochellière, François Brouillette, Patrick Lévesque, Nicolas Dognin, Raphaël St-Germain, Goran Rimac, Sylvain Lemay, François Philippon, Mario Sénéchal
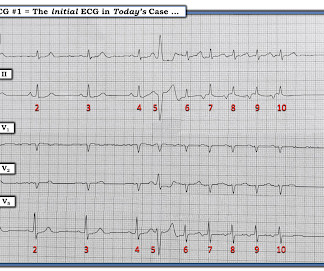
First, we have a narrow-complex, regular tachycardia, with a rate of about 135-140. This narrows our differential for the rhythm down to sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT, or SVT), and atrialflutter. They are flutter waves, and the rhythm is 2:1 atrialflutter.
RBBB is no longer seen after conversion to sinus rhythm — which supports our suspicion that the intermittent RBBB conduction seen every-other-beat during the tachycardia ( in Figure-1 ) was rate-related. Note that QRS morphology after conversion to sinus rhythm is very similar to QRS morphology of odd-numbered beats during the tachycardia.
Cheng and Zhang to our paper1, we note that despite ARVC being a relatively uncommon cardiomyopathy, we uniquely report on a large clinical experience with very long-term follow-up after VT ablation and confirm a high incidence of atrialflutter (AFL) and the effectiveness and low risk of catheter ablation of AFL.
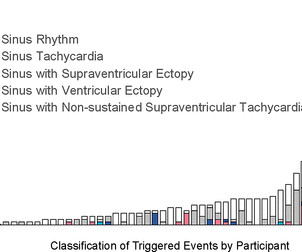
No participant demonstrated atrial fibrillation, atrialflutter, sustained supraventricular tachycardia (SVT), sustained ventricular tachycardia or infranodal atrioventricular block. Median monitoring duration was 13.2 (IQR Nearly all participants (96%) had an ectopic burden of <1%; one participant had a 2.8%
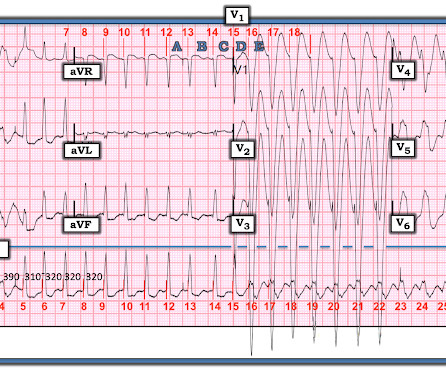
Are the wide complexes due to a supraventricular rhythm (AVNRT or Atrialflutter or atrial fib) with aberrancy? Or are they due to ventricular tachycardia (VT). The rhythm alternates between a wide complex (first 4 beats, and beats 16-28) and narrow complex (beats 5-15). There are no P-waves. Sinus P waves are absent.
Sinus tachycardia – sinus rhythm above 100 bpm is a sinus tachycardia. Ventricular tachycardia – more than 7 consecutive complexes originating from ventricles at a rate of > 100 bpm. Supraventricular tachycardia – more than 7 consecutive complexes of supraventricular beats at a rate of > 100 bpm.
In all probability, this dilation is a form of atrialtachycardia and atrial cardiomyopathy. However, underlying lesions such as hypertension, mitral valve disease, COPD, ASD, and TR greatly influence the degree of atrial enlargement. We know atrialflutters can be confined to one atrium.
The rhythm is indeed irregularly irregular, so atrial fibrillation must be considered. There are 5 other rhythms that are irregularly irregular , though atrial fibrillation is by far the most common: 1. Multifocal AtrialTachycardia 2. Sinus with multifocal PACs 3. Sinus with multifocal PVCs 4.
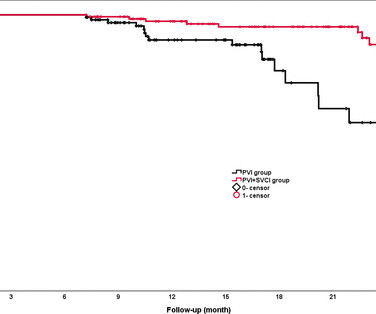
Regular clinical follow-ups were conducted to detect AF recurrence, defined as any episode of atrial fibrillation, atrialflutter or atrialtachycardia lasting >30 s. RFCA was guided by quantitative AI in both groups.
There are 2 atrial "bumps" for every QRS. Here I put arrows: Arrows shows slow atrialflutter waves. The PEARL is that recognition of a longer-than-expected P wave in a supraventricular tachycardia should bring to mind the “Bix Rule” ( See My Comment at the bottom of the page in the August 3, 2018 post in Dr. Smith's ECG Blog ).
Abstract Introduction Atrial fibrillation and atrialflutter originating from the donor s heart is a commonly reported complication post heart transplant. Case A 47-year-old male presented with atrialtachycardia 6 months post heart transplant.
Available study and registry data as well as case reports concerning utilization of the QDOT MICRO™ Catheter for the treatment of cardiac arrhythmias including AF, focal and macroreentry atrialtachycardia, typical atrialflutter by cavotricuspid isthmus block, premature ventricular contractions, and accessory pathways were reviewed and summarized.
Abstract Introduction The use of flecainide and propafenone for medical cardioversion of atrial fibrillation (AF) and atrialflutter/intra-atrial reentrant tachycardia (IART) is well-described in adults without congenital heart disease (CHD).
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrialflutter with regular conduction. There are no P waves preceding the QRS complexes, and no clear flutter waves.
This study aimed to evaluate a short-term anti-inflammatory treatment with colchicine following ablation of AF.METHODS:Patients scheduled for ablation were randomized to receive colchicine 0.6 mg twice daily or placebo for 10 days. The first dose of the study drug was administered within 4 hours before ablation.
By this definition, a variety of rhythms may qualify as “SVTs” — including sinus tachycardia, atrialflutter or fibrillation, MAT, AVRT/AVNRT, among others. Why Isn’t this a Run of AtrialTachycardia? — ECG Blog #138 — AFlutter vs AtrialTachycardia.
On the other hand, non-FAAM-guided ablation was performed via linear ablation, complex fractionated atrial electrogram ablation, superior vena cava isolation, and focal ablation according to the location of the non-PV foci. The primary endpoints were AF recurrence, atrialflutter, and/or atrialtachycardia.
PEARL # 3: AtrialFlutter with 1:1 AV conduction is rare! Since the rate of atrial activity with flutter in adults is most often very close to 300 /minute ( ie, usual range for atrial activity ~250-350/minute ) — AFlutter with 2:1 AV conduction typically results in a regular ventricular rate of ~140-160/minute.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content