This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
male with pertinent past medical history including Atrial fibrillation, atrialflutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Bedside ultrasound showed volume depletion and no pulmonary edema.
Patients in the study will be randomized to undergo pulmonary vein isolation (PVI) and left atrial posterior wall ablation using the FARAPULSE PFA System, or receive AAD treatment, and followed for three years. The randomized AVANT GUARD trial will enroll more than 500 patients diagnosed with persistent AF at up to 75 sites globally.
Both atria develop from a combination of the primitive atrium, sinus venous, and pulmonary veins.It In all probability, this dilation is a form of atrialtachycardia and atrial cardiomyopathy. Pulmonary veins have been the primary target for ablation for many years, yet the success rates remain inconsistent.
She was noted to be in heart failure, with hypotension and tachycardia. Echocardiography demonstrated severe calcific mitral stenosis with pulmonary hypertension. She reverted to normal sinus rhythm with features of left atrial enlargement, a heart rate of 60/min and a prolonged corrected QT interval (474 ms) ( figure 1B ).
There is a narrow complex tachycardia at a rate of 130. ECGs: there is a regular narrow complex tachycardia still at a rate of exactly 130, with no P-waves and also no change since the prehospital ECG. Leads II and aVF appear to have flutter waves. I diagnosed atrialflutter with 2:1 conduction. Is is sinus?
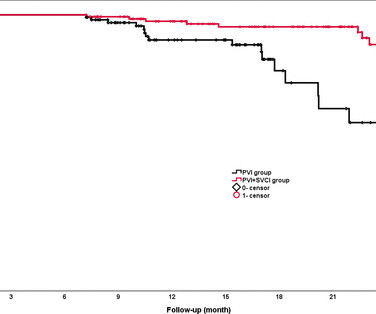
Background The value of empirical superior vena cava isolation (SVCI) following pulmonary vein isolation (PVI) to improve the efficacy of radiofrequency catheter ablation (RFCA) for paroxysmal atrial fibrillation (PAF) remains controversial. RFCA was guided by quantitative AI in both groups.
The rhythm is indeed irregularly irregular, so atrial fibrillation must be considered. There are 5 other rhythms that are irregularly irregular , though atrial fibrillation is by far the most common: 1. Multifocal AtrialTachycardia 2. Sinus with multifocal PACs 3. Sinus with multifocal PVCs 4. GET a 12-lead!
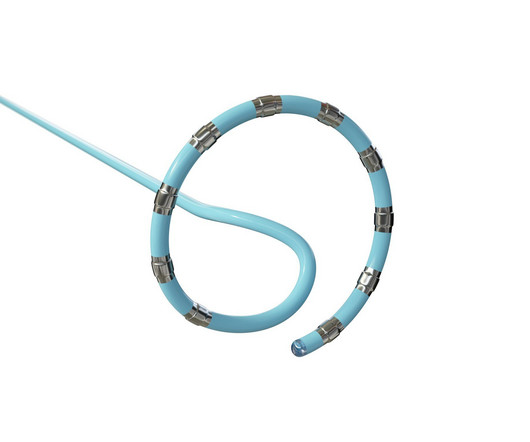
Although the QDOT MICRO™ Catheter was mainly designed for pulmonary vein isolation (PVI) its versatility to treat atrial fibrillation (AF) and other types of arrhythmias was recently evaluated by the FAST and FURIOUS study series and other studies and will be presented in this article.
FAAM ablation successfully decreased the recurrence rate of atrial tachyarrhythmia compared with conventional non-PV foci ablation. Abstract Introduction Treatment of recurrent atrial fibrillation (AF) is sometimes challenging due to non-pulmonary vein (PV) foci. The RHYTHMIA system was used to perform all the procedures.
The bedside echo showed a large RV (Does this mean there is a pulmonary embolism as the etiology?) The rhythm is 2:1 atrialflutter. The flutter waves can conceal or mimic ischemic repolarization findings, but here I don't see any obvious findings of OMI or subendocardial ischemia. Lots of info here.
Here is his 12-lead ECG: The computer reads supraventricular tachycardia. It is atrialflutter with 2:1 conduction. There are clear flutter waves in lead II across the bottom. Adenosine simply blocks the AV node so that there is no QRS to hide the flutter waves, and they become obvious. What is it?
2** Furthermore, the primary effectiveness endpoint (PEE) of acute pulmonary vein isolation and 12-month freedom from atrial arrhythmia recurrence (AF, AtrialTachycardia, or AtrialFlutter) was 75.6%. Pulsed Field Ablation for Pulmonary Vein Isolation in Atrial Fibrillation. Catheter Ablation.
This prospective, multicenter study conducted in the United States, Italy, and China investigated the safety and efficacy of pulmonary vein isolation (PVI) using HELIOSTAR in drug-refractory symptomatic PAF. The primary safety endpoint was the occurrence of early-onset primary adverse events (PAEs).
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Serious outcomes included death, arrhythmia, myocardial infarction, structural heart disease, pulmonary embolism, and hemorrhage.
ABSTRACT Introduction Freedom from recurrences of atrial tachyarrhythmia (ATA) is suboptimal after pulmonary vein isolation (PVI) in patients with persistent atrial fibrillation (PsAF). Univariate and multivariable Cox regression analysis (with ATA recurrence as an endpoint) was performed to identify CBA responders.
Smith comments : Wide complex tachycardia. The differential diagnosis of WCT is: 1) Sinus tachycardia with "aberrancy" (in this case RBBB and LAFB), but there are no P-waves and the QRS morphology is not typical of simple RBBB/LAFB. Also, if the rate is constant, not wavering up and down, it is highly unlikely to be sinus tachycardia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content