This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
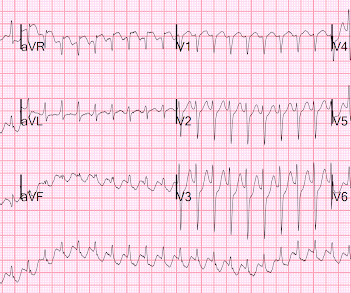
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. The ECG was interpreted as showing atrialflutter with 2:1 conduction. Are you confident there is no ischemia? Answer : The ECG above shows a regular wide complex tachycardia. The ECG below was recorded. Is this: 1.
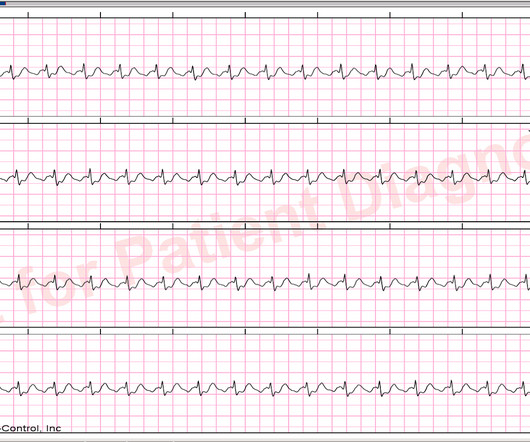
So it is not atrial fib and not VT. It is a regular narrow complex tachycardia. There is a lot of ST depression -- this is ischemia caused by the very fast rate and is an indication for emergent electrical cardioversion. If you look closely at lead II across the bottom, it appears there are flutter waves. What is the DDx?
The rhythm differential for narrow, regular, and tachycardic is sinus rhythm, SVT (encompassing AVNRT, AVRT, atrial tach, etc), and atrialflutter (another supraventricular rhythm which is usually considered separately from SVTs). Therefore this patient is either in some form of SVT or atrialflutter.
Here is his initial rhythm strip (it is not a full 10 seconds): Wide complex tachycardia, rate 235 This is a very wide complex regular tachycardia at a rate of 235. It should be considered to be Ventricular Tachycardia and treated as such. Rate 120, flutter rate 240. ACS is of course possible. Still more ST depression.
There is the appearance of STE in inferior leads II, III, and aVF (with STD in aVR), but this is entirely due to flutter waves which are only seen in those leads. Also, the atrialflutter in this case is relatively slow like in many other cases we've shown. Tachycardia and ST Elevation. AtrialFlutter with Inferior STEMI?
At about this point in the process — I like to take a closer LOOK at the 12-lead tracing, to ensure there is no acute ischemia or infarction that might need immediate attention. PEARL # 3: At this point — the most time-efficient step for solving today's rhythm will be to determine the nature of atrial activity.
There is a narrow complex tachycardia at a rate of 130. ECGs: there is a regular narrow complex tachycardia still at a rate of exactly 130, with no P-waves and also no change since the prehospital ECG. Leads II and aVF appear to have flutter waves. I diagnosed atrialflutter with 2:1 conduction. Is is sinus?
First, we have a narrow-complex, regular tachycardia, with a rate of about 135-140. This narrows our differential for the rhythm down to sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT, or SVT), and atrialflutter. They are flutter waves, and the rhythm is 2:1 atrialflutter.
Here I put arrows: Arrows shows slow atrialflutter waves. The problem is, that the PR interval of the upright deflection in lead II ( under the RED arrows ) is relatively long ( clearly more than 1 large box in duration ) — and if anything, the PR interval should shorten when there is tachycardia. These mimic ST Elevation.
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrialflutter with regular conduction. There are no P waves preceding the QRS complexes, and no clear flutter waves.
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below. Arch Intern Med.
The rhythm is 2:1 atrialflutter. The flutter waves can conceal or mimic ischemic repolarization findings, but here I don't see any obvious findings of OMI or subendocardial ischemia. The rhythm in ECG #1 is not Sinus Tachycardia — because there is no upright P wave in lead II. Lots of info here.
Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. There is a large peaked P-wave in lead II (right atrial enlargement) There is left axis deviation consistent with left anterior fascicular block. There is no evidence of infarction or ischemia. So what is it?
No evidence for ischemia jumps out. Additionally, the patient had no other apparent reason to have sinus tachycardia (such as volume depletion, bleeding, fever). So the most likely rhythm in ECG 1 is ectopic atrialtachycardia. Therefore the first part of ECG 1 shows ectopic atrialtachycardia with biventricular pacing.
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Evidence of acute ischemia (may be subtle) vii. Most physicians will automatically be worried about these symptoms. Left BBB vi.
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). That said there were no clinical symptoms or ECG findings suggestive of ongoing ischemia. This patient very likely has some form of idiopathic ventricular tachycardia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content