This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
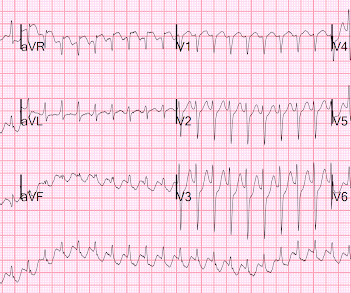
There is the appearance of STE in inferior leads II, III, and aVF (with STD in aVR), but this is entirely due to flutter waves which are only seen in those leads. Also, the atrialflutter in this case is relatively slow like in many other cases we've shown. AtrialFlutter with Inferior STEMI? Is this inferor STEMI?
Written by Jesse McLaren A 65 year old with a history of atrialflutter, CABG and end-stage renal disease on dialysis presented with 3 days of fluctuating chest pain, which was ongoing at triage. The first ECG was labeled “anterior subendocardial ischemia”, but subendocardial ischemia does not localize. What do you think?
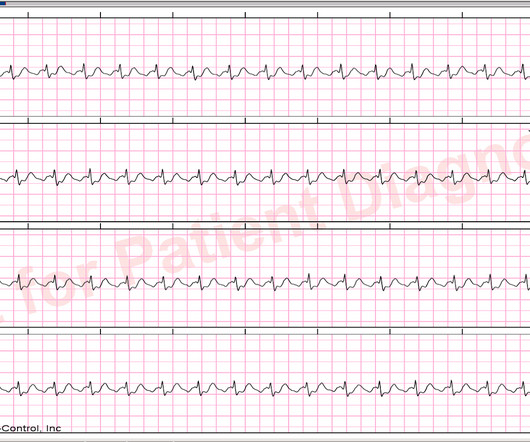
There is a lot of ST depression -- this is ischemia caused by the very fast rate and is an indication for emergent electrical cardioversion. The fact that the patient is on Flecainide and Diltiazem is good evidence that this is atrialflutter with 1:1 conduction. This is atrialflutter with 1:1 conduction.
If it is slow Atrialflutter with 1:1 conduction, it should slow the conduction and reveal the flutter waves. This is the exact rate one expects with slow atrialflutter and it is why slow atrialflutter can be so dangerous: it conducts 1:1, with fast ventricular rates. Rate 120, flutter rate 240.
The ECG was interpreted as showing atrialflutter with 2:1 conduction. Are you confident there is no ischemia? The heart rate could be compatible with that of a 2:1 conducted atrialflutter. Also, lead I could give the initial impression of showing flutter waves. Do you agree with this strategy?
This narrows our differential for the rhythm down to sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT, or SVT), and atrialflutter. The patient’s history is notable for paroxysmal atrial fibrillation, which raises clinical suspicion for atrialflutter, since these two entities frequently coexist on a spectrum.
If this STD were due to LVH or to subendocardial ischemia, rather than posterior OMI, it would be maximal in V5 and V6. By itself these would not be diagnostic as they do not have typical morphology (flat T-waves, possible atrial repolarization wave to account for ST depression). ng/mL, and another ECG was recorded and was identical.
My interpretation was: RBBB with hyperacute T-waves in V4-V6 that are all but diagnostic of LAD occlusion vs. post ROSC ischemia. The patient had ROSC and maintained it. A 12-lead ECG was obtained: What do you think? Regional wall motion abnormality--apical anterior, mid anteroseptal, apical septal, and apical inferior akinesis.
Here I put arrows: Arrows shows slow atrialflutter waves. These mimic ST Elevation. But there is no STE. Of course the Queen knows it is not OMI: Click here to sign up for Queen of Hearts Access Here are other cases of the same: A 50 year old man with sudden altered mental status and inferior STE. Would you give lytics? Arrhythmia?
Re-entrant tachycardias (atrialflutter, PSVT, AVRT, VT) have constant regular heart rates, whereas sinus tachycardia will usually gradually change rate with differing conditions (for instance, after infusion of fluid and BP increase, sinus tach rate might decrease from 130 to 125, for instance). So there is a re-entrant rhythm.
At about this point in the process — I like to take a closer LOOK at the 12-lead tracing, to ensure there is no acute ischemia or infarction that might need immediate attention. PEARL # 3: At this point — the most time-efficient step for solving today's rhythm will be to determine the nature of atrial activity.
The rhythm is 2:1 atrialflutter. The flutter waves can conceal or mimic ischemic repolarization findings, but here I don't see any obvious findings of OMI or subendocardial ischemia. The bedside echo showed a large RV (Does this mean there is a pulmonary embolism as the etiology?) Lots of info here.
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrialflutter with regular conduction. There are no P waves preceding the QRS complexes, and no clear flutter waves.
The Differential Diagnosis is: SVT with aberrancy(#) [AVNRT vs. WPW (also called AVRT*)] Atrialflutter with 1:1 conduction, with aberrancy VT coming from the anterior fascicle ( fascicular VT )@ *AVRT = AV Reciprocating Tachycardia (Tachycardic loop that uses both the AV node and an accessory pathway.
Atrialflutter with 2:1 conduction. The atrialflutter rate is approximately 200 bpm, with 2:1 AV conduction resulting in ventricular rate almost exactly 100 bpm. Further history revealed she had new onset atrialflutter soon after her aortic surgery, and was put on flecainide approximately 1 month ago.
The rhythm differential for narrow, regular, and tachycardic is sinus rhythm, SVT (encompassing AVNRT, AVRT, atrial tach, etc), and atrialflutter (another supraventricular rhythm which is usually considered separately from SVTs). Therefore this patient is either in some form of SVT or atrialflutter.
There is a large peaked P-wave in lead II (right atrial enlargement) There is left axis deviation consistent with left anterior fascicular block. There is no evidence of infarction or ischemia. There is atrial activity before every QRS, but that activity has negative polarity, so it is not sinus rhythm.
LAFB, atrialflutter, anterolateral STEMI(+) OMI. EKG shown here: LAFB with no clear signs of OMI or ischemia. At 20 minutes from initial ECG, the patient's native rhythm spontaneously usurped the rhythm from the pacemaker: No knowledge or guidelines needed to see the OMI findings now! No labs were performed.
Evidence of acute ischemia (may be subtle) vii. ST segment and T wave abnormalities consistent with or possibly related to myocardial ischemia. And these findings come from OESIL , EGSYS , and Sarasin studies: i: Non-sinus rhythm ii: SVT or VT (obviously, and this makes for an abnormal vital sign anyway) iii. Left BBB vi. LVH or RV d.
No evidence for ischemia jumps out. Cardioversion is most beneficial for reentrant arrhythmias ( e.g. VT, atrialflutter, AVNRT, atrial fibrillation) because it terminates the reentry circuit. He said he had had three episodes of chest pain that day while urinating. ECG 1 What do you think?
That said there were no clinical symptoms or ECG findings suggestive of ongoing ischemia. You have given IV MgSO4 a fast acting -blocker and IV amiodarone bolus and infusion. The possibility of an ischemic cause of the ventricular arrhythmia has to be considered! Troponin T was negative on admission and on repeat blood draw.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content