This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Head CT scans showed hypoattenuating areas indicative of cerebral infarction, chest CT suggested possible air accumulation in the left atrial region. ECG findings were consistent with atrialflutter, myocardial infarction, and incomplete right bundle branch block.
ABSTRACT Atrialflutter (AFL), defined as macro-re-entrant atrial tachycardia, is associated with debilitating symptoms, stroke, heartfailure, and increased mortality. AFL is classified into typical, or cavotricuspid isthmus (CTI)-dependent, and atypical, or non-CTI-dependent.
Wild-type transthyretin amyloid cardiomyopathy (ATTRwt-CM) is often accompanied by atrial fibrillation (AF), atrialflutter (AFL), and atrial tachycardia (AT), which are difficult to control because beta-blockers and antiarrhythmic drugs can worsen heartfailure (HF).
A fully upright P-wave is typical atrial activity of atrialflutter as seen in V1. See these example cases of upright P-waves: Case Continued Thus, I was all but certain that this was atrialflutter. Smith — the choice of IV Digoxin was appropriate and effective in today's case.
Early treatment of persistent AF can reduce the risk of blood clots, stroke, and heartfailure, and may prevent the disease from becoming permanent. Patients are often treated with AADs as frontline therapy for heart rhythm maintenance, though some can experience adverse effects and limited efficacy.
She was noted to be in heartfailure, with hypotension and tachycardia. With decompensated heartfailure and adequate prior anticoagulation, the patient underwent direct current synchronised cardioversion for her arrhythmia. Echocardiography demonstrated severe calcific mitral stenosis with pulmonary hypertension.
The ECG was interpreted as showing atrialflutter with 2:1 conduction. The heart rate is about 130 bpm. The heart rate could be compatible with that of a 2:1 conducted atrialflutter. Also, lead I could give the initial impression of showing flutter waves. The ECG below was recorded.
Cardioversion is used to correct abnormal heart rhythms, also known as arrhythmias. When your heart beats too quickly, too slow, or irregularly, it can affect your blood flow and lead to severe complications like stroke or heartfailure. Cardioversions can help “reset” your heart rhythm to its regular pattern.
The rhythm is 2:1 atrialflutter. The flutter waves can conceal or mimic ischemic repolarization findings, but here I don't see any obvious findings of OMI or subendocardial ischemia. The bedside echo showed a large RV (Does this mean there is a pulmonary embolism as the etiology?) Here is his triage ECG: What do you think?
The patient has heartfailure as a result of this event. 2 months later, he presented in pulmonary edema with atrialflutter and formal echo had EF 20% Why did this happen? How could an occlusion (Occlusion MI, OMI) that results in the loss of a massive amount of myocardium and results in HeartFailure be missed?
NT-proBNP values less than 300 pg/ml have a 99% negative predictive value for excluding congestive heartfailure. A cutoff of 1200 pg/ml for patients with a normal eGFR is very specific for heartfailure. There is atrial activity before every QRS, but that activity has negative polarity, so it is not sinus rhythm.
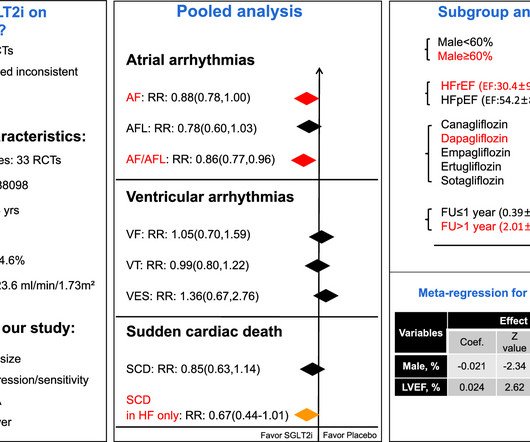
The effects of SGLT2i on atrial fibrillation(AF), atrialflutter(AFL), composite AF/AFL, ventricular fibrillation(VF), ventricular tachycardia(VT), ventricular extrasystoles(VES), sudden cardiac death(SCD) and composite VF/VT/SCD were evaluated. SGLT2i lowers the risk of SCD only in heartfailure patients.
Methods The primary effectiveness endpoint (PEE) was 12-month freedom from documented atrial fibrillation/atrialflutter/atrial tachycardia plus freedom from acute procedural failure, nonstudy catheter failure, repeat ablation failure, direct current cardioversion (DCCV), and Class I/III antiarrhythmic drug (AAD) failure.
History of Cardiovascular disease (all studies): Especially any history of heartfailure or structural cardiac disease, including valvular 4. to 22.7), a history of congestive heartfailure (OR: 5.3, Age greater than 65 (Sarasin and STePS) 3. Syncope without a prodrome, no precipitating factors (EGSYS) 5. 95% CI = 1.9
ABSTRACT Typical atrialflutter (AFL), defined as cavotricuspid isthmus (CTI)-dependent macro-re-entrant atrial tachycardia, often causes debilitating symptoms, and is associated with increased incidence of atrial fibrillation, stroke, heartfailure, and death.
Possible but, again, the QRS morphology is atypical 3) AtrialFlutter with 2:1 conduction and "aberrancy". I do not see flutter wave baseline, and again the QRS morphology is not typical for a supraventricular rhythm. See this case, for example: A Relatively Narrow Complex Tachycardia at a Rate of 180.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content