This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
QUESTIONS: Is this rhythm too fast to be sinus tachycardia? Are flutter waves hidden within the QRS and T waves? I say this for the simple reason that to pick any of the above 4 choices — is to imply with 100% certainty that you know the answer ( or, as is implied in the title of today’s Blog post — this would be premature closure).
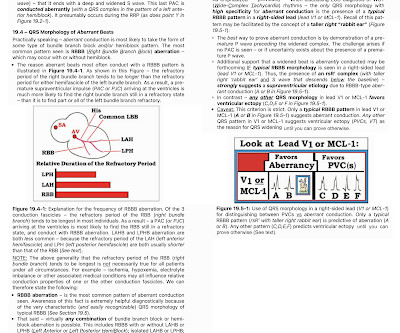
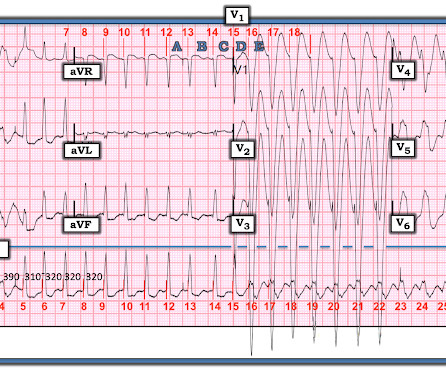
By the P s, Q s, 3 R Approach ( See ECG Blog #185 ): The rhythm is fast and QRS complexes are R egular. PEARL # 4: As emphasized in ECG Blog #204 , in which I review derivation of the bundle branch blocks — RBBB is a terminal conduction delay. Figure-2: I've labeled the initial ECG in today's case. And a Final Tracing.
With experience, applying the P s, Q s, 3 R Approach ( See ECG Blog #185 ) — to formulate the above steps in our initial assessment of the rhythm in Figure-1 can ( should ) be completed in less than 30 seconds! These are reviewed in ECG Blog #343. I reviewed the concept of Echo beats in ECG Blog #239.
male with pertinent past medical history including Atrial fibrillation, atrialflutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Description : Regular Wide Complex Tachycardia at a rate of about 160.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. The ECG was interpreted as showing atrialflutter with 2:1 conduction. Answer : The ECG above shows a regular wide complex tachycardia. The heart rate could be compatible with that of a 2:1 conducted atrialflutter.
There is a regular narrow complex tachycardia. Thus, it is supraventricular tachycardia. It is important to remember that SVT includes Sinus Tachycardia! See many cases with use of Lewis Leads on this blog: Case continued The providers jumped to conclusions and gave adenosine. His pulse was 186. I do not have the strips.
As discussed in detail in ECG Blog #240 — the term, “SVT” — refers to any supraventricular rhythm (ie, with origin at or above the AV node ) that manifests a rate of ≥100/minute. By this definition, a variety of rhythms may qualify as “SVTs” — including sinus tachycardia, atrialflutter or fibrillation, MAT, AVRT/AVNRT, among others.
NOTE: The ECG in Figure-1 has been recorded at the usual 25mm/second speed — but with the Cabrera format ( Please see my Editorial Note near the top of the page in ECG Blog #365 for review of the basics of this recording system ). PEARL # 3: AtrialFlutter with 1:1 AV conduction is rare! ECG Blog #287 — More on AFlutter.
As always — I like to start by focusing on the long lead rhythm strip — which shows a bigeminal rhythm — in that there are repetitive 2-beat groups ( See ECG Blog #232 for review of the concept of “bigeminy” ). PEARL # 1: As discussed in ECG Blog #232 — it helps to consider the differential diagnosis of a bigeminal rhythm.
There is a regular wide complex tachycardia. A fully upright P-wave is typical atrial activity of atrialflutter as seen in V1. See these example cases of upright P-waves: Case Continued Thus, I was all but certain that this was atrialflutter. If it is flutter, it will reveal the underlying flutter waves.
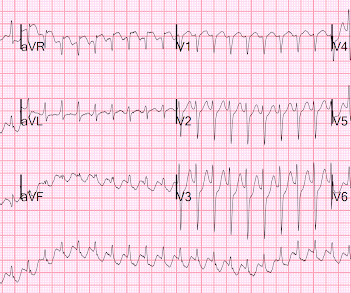
Here is his initial rhythm strip (it is not a full 10 seconds): Wide complex tachycardia, rate 235 This is a very wide complex regular tachycardia at a rate of 235. It should be considered to be Ventricular Tachycardia and treated as such. Rate 120, flutter rate 240. Still more ST depression. So what happened?
So it is not atrial fib and not VT. It is a regular narrow complex tachycardia. The fact that the patient is on Flecainide and Diltiazem is good evidence that this is atrialflutter with 1:1 conduction. If you look closely at lead II across the bottom, it appears there are flutter waves. What is the DDx?
Wide-complex tachycardia: VT or aberrant, or "other?" The patient had a history of paroxysmal atrial fibrillation and several cardioversions. A wide-complex tachycardia in an older patient must immediately suggest ventricular tachycardia. Instead, the rate of 150, plus the history of AF, suggested atrialflutter.
Initial ECG in the ED: Presenting ECG : Wide-complex tachycardia at a rate about 200. This is overwhelmingly likely to be ventricular tachycardia, even if only age and medical history are considered. Nevertheless, the widths of both the QRS complex and the RS duration are similar in both the old ECG and the tachycardia.
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? To me, it was clearly atrialflutter with 1:1 conduction. The rate of 280 is just right for atrialflutter. The waves look like atrialflutter waves, NOT like a wide ventricular complex.
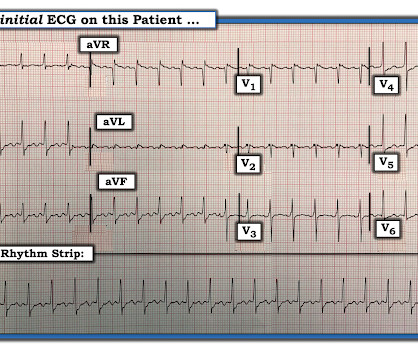
Here is his 12-lead ECG: The computer reads supraventricular tachycardia. It is atrialflutter with 2:1 conduction. There are clear flutter waves in lead II across the bottom. Adenosine simply blocks the AV node so that there is no QRS to hide the flutter waves, and they become obvious. What is it?
There is the appearance of STE in inferior leads II, III, and aVF (with STD in aVR), but this is entirely due to flutter waves which are only seen in those leads. Also, the atrialflutter in this case is relatively slow like in many other cases we've shown. Tachycardia and ST Elevation. AtrialFlutter with Inferior STEMI?
The rhythm differential for narrow, regular, and tachycardic is sinus rhythm, SVT (encompassing AVNRT, AVRT, atrial tach, etc), and atrialflutter (another supraventricular rhythm which is usually considered separately from SVTs). Therefore this patient is either in some form of SVT or atrialflutter.
First, we have a narrow-complex, regular tachycardia, with a rate of about 135-140. This narrows our differential for the rhythm down to sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT, or SVT), and atrialflutter. They are flutter waves, and the rhythm is 2:1 atrialflutter.
There is a narrow complex tachycardia at a rate of 130. ECGs: there is a regular narrow complex tachycardia still at a rate of exactly 130, with no P-waves and also no change since the prehospital ECG. Leads II and aVF appear to have flutter waves. I diagnosed atrialflutter with 2:1 conduction. Is is sinus?
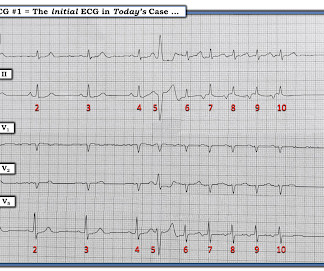
There are 2 atrial "bumps" for every QRS. Here I put arrows: Arrows shows slow atrialflutter waves. I favor the P s, Q s, 3 R Approach — as a simple acronym to facilitate recall of the 5 KEY Parameters for rhythm interpretation ( See My Comment in the October 25, 2022 post in Dr. Smith’s ECG Blog ). Look at V1.
Are the wide complexes due to a supraventricular rhythm (AVNRT or Atrialflutter or atrial fib) with aberrancy? Or are they due to ventricular tachycardia (VT). The rhythm alternates between a wide complex (first 4 beats, and beats 16-28) and narrow complex (beats 5-15). There are no P-waves. Sinus P waves are absent.
The rhythm is indeed irregularly irregular, so atrial fibrillation must be considered. There are 5 other rhythms that are irregularly irregular , though atrial fibrillation is by far the most common: 1. Multifocal AtrialTachycardia 2. Sinus with multifocal PACs 3. Sinus with multifocal PVCs 4.
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrialflutter with regular conduction. There are no P waves preceding the QRS complexes, and no clear flutter waves.
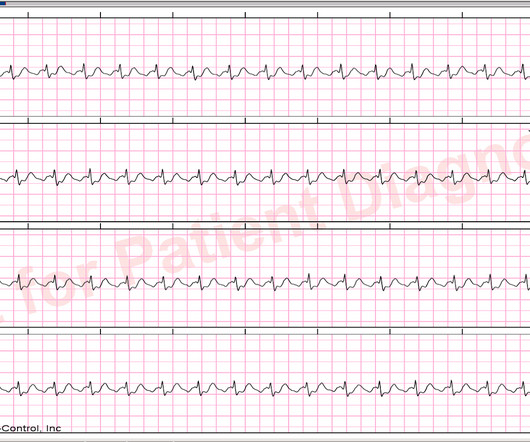
M y A pproach to this R hythm : I reviewed the basics for rhythm interpretation in the October 16, 2019 Case from Dr. Smith’s ECG Blog. L ooking f or F lutter W aves : The diagnosis of AFlutter can be established in a regular SVT at ~150/minute — IF you are able to identify regular atrial activity at ~300/minute.
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below. Arch Intern Med.
The rhythm is 2:1 atrialflutter. The flutter waves can conceal or mimic ischemic repolarization findings, but here I don't see any obvious findings of OMI or subendocardial ischemia. The rhythm in ECG #1 is not Sinus Tachycardia — because there is no upright P wave in lead II. Here is his triage ECG: What do you think?
Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. There is a large peaked P-wave in lead II (right atrial enlargement) There is left axis deviation consistent with left anterior fascicular block. See my quick review of atrialtachycardia below) The tachycardia spontaneously resolved.
Additionally, the patient had no other apparent reason to have sinus tachycardia (such as volume depletion, bleeding, fever). So the most likely rhythm in ECG 1 is ectopic atrialtachycardia. Therefore the first part of ECG 1 shows ectopic atrialtachycardia with biventricular pacing. Point 1: What is PVARP?
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Most physicians will automatically be worried about these symptoms. The tracings were considered abnormal in the following cases: 1.
Smith comments : Wide complex tachycardia. The differential diagnosis of WCT is: 1) Sinus tachycardia with "aberrancy" (in this case RBBB and LAFB), but there are no P-waves and the QRS morphology is not typical of simple RBBB/LAFB. Also, if the rate is constant, not wavering up and down, it is highly unlikely to be sinus tachycardia.
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). The intricacies of the different classes of antiarrhythmics and their mechanism of action extend beyond the scope of this blog. Potassium and magnesium serum levels were normal.
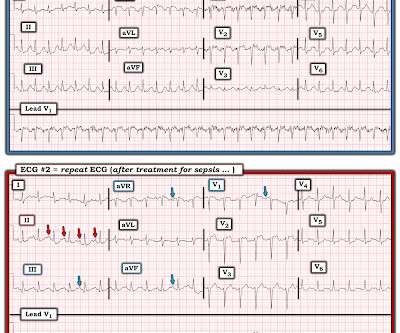
Figure-1: While at first glance the rhythm in Figure-1 might be mistaken for sinus tachycardia in fact, this is not the rhythm. Instead there is 2:1 atrial activity that is best seen in lead V1 ( See Figure-2 ). However, having noticed the 2:1 atrial activity in lead V1 I was not at all convinced that the episode was VT.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content