This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
I say this for the simple reason that to pick any of the above 4 choices — is to imply with 100% certainty that you know the answer ( or, as is implied in the title of today’s Blog post — this would be premature closure). ECG Blog #240 — The regular SVT. ECG Blog #229 — Why is AFlutter so commonly overlooked? s in Figure-2 ).
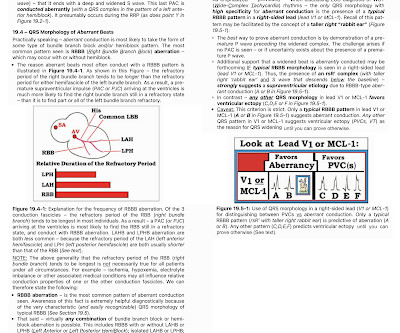
By the P s, Q s, 3 R Approach ( See ECG Blog #185 ): The rhythm is fast and QRS complexes are R egular. PEARL # 4: As emphasized in ECG Blog #204 , in which I review derivation of the bundle branch blocks — RBBB is a terminal conduction delay. ECG Blog #185 — Reviews the P s, Q s, 3 R Approach to Rhythm Interpretation.
NOTE: The ECG in Figure-1 has been recorded at the usual 25mm/second speed — but with the Cabrera format ( Please see my Editorial Note near the top of the page in ECG Blog #365 for review of the basics of this recording system ). PEARL # 3: AtrialFlutter with 1:1 AV conduction is rare! ECG Blog #287 — More on AFlutter.
As discussed in detail in ECG Blog #240 — the term, “SVT” — refers to any supraventricular rhythm (ie, with origin at or above the AV node ) that manifests a rate of ≥100/minute. By this definition, a variety of rhythms may qualify as “SVTs” — including sinus tachycardia, atrialflutter or fibrillation, MAT, AVRT/AVNRT, among others.
As always — I like to start by focusing on the long lead rhythm strip — which shows a bigeminal rhythm — in that there are repetitive 2-beat groups ( See ECG Blog #232 for review of the concept of “bigeminy” ). PEARL # 1: As discussed in ECG Blog #232 — it helps to consider the differential diagnosis of a bigeminal rhythm.
With experience, applying the P s, Q s, 3 R Approach ( See ECG Blog #185 ) — to formulate the above steps in our initial assessment of the rhythm in Figure-1 can ( should ) be completed in less than 30 seconds! These are reviewed in ECG Blog #343. I reviewed the concept of Echo beats in ECG Blog #239.
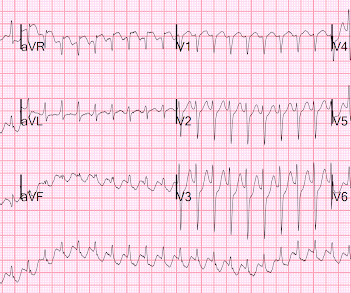
A fully upright P-wave is typical atrial activity of atrialflutter as seen in V1. See these example cases of upright P-waves: Case Continued Thus, I was all but certain that this was atrialflutter. I'd add the following thoughts to Dr. Smith's discussion.
If it is slow Atrialflutter with 1:1 conduction, it should slow the conduction and reveal the flutter waves. This is the exact rate one expects with slow atrialflutter and it is why slow atrialflutter can be so dangerous: it conducts 1:1, with fast ventricular rates. Rate 120, flutter rate 240.
To me, it was clearly atrialflutter with 1:1 conduction. The rate of 280 is just right for atrialflutter. The waves look like atrialflutter waves, NOT like a wide ventricular complex. Reverted to atrial fibrillation with RVR while in the hospital 3 times and needed cardioversion.
- PSVT (which includes AVNRT and orthodromic AV reciprocating tachycardia) [AVRT uses an accessory pathway, a "bypass tract" and thus is seen in WPW; about 30% of PSVT is orthodromic AVRT] - AtrialFlutter with 1:1 conduction. If you look closely at lead II across the bottom, it appears there are flutter waves. Which is it?
There is the appearance of STE in inferior leads II, III, and aVF (with STD in aVR), but this is entirely due to flutter waves which are only seen in those leads. Also, the atrialflutter in this case is relatively slow like in many other cases we've shown. AtrialFlutter with Inferior STEMI? Is this inferor STEMI?
This narrows our differential for the rhythm down to sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT, or SVT), and atrialflutter. The patient’s history is notable for paroxysmal atrial fibrillation, which raises clinical suspicion for atrialflutter, since these two entities frequently coexist on a spectrum.
The ECG was interpreted as showing atrialflutter with 2:1 conduction. The heart rate could be compatible with that of a 2:1 conducted atrialflutter. Also, lead I could give the initial impression of showing flutter waves. I have emphasized on many occasions in Dr. Smith's ECG Blog how AFlutter is by far (!)
Written by Jesse McLaren A 65 year old with a history of atrialflutter, CABG and end-stage renal disease on dialysis presented with 3 days of fluctuating chest pain, which was ongoing at triage. What do you think? Do you need posterior leads?
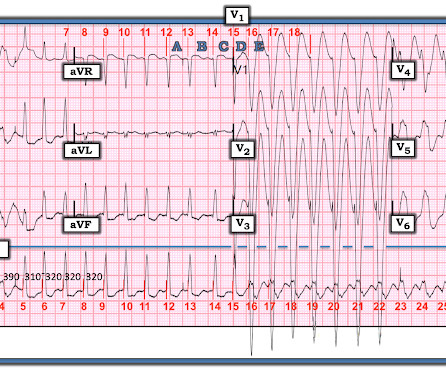
The WCT is interrupted by a series of variable-morphology QRS complexes, with atrialflutter waves note in II, III, and aVF. Detail of Flutter waves The rate of the flutter waves matches the rate of the WCT (about 200/m), proving that the presenting WCT had been 1:1 atrialflutter.
Instead, the rate of 150, plus the history of AF, suggested atrialflutter. A close inspection of lead II showed P or flutter waves at a rate of about 300 bpm, also supporting atrialflutter. There appear to be flutter waves at a rate of 300. Flecainide encourages new atrialflutter.
There are 2 atrial "bumps" for every QRS. Here I put arrows: Arrows shows slow atrialflutter waves. I favor the P s, Q s, 3 R Approach — as a simple acronym to facilitate recall of the 5 KEY Parameters for rhythm interpretation ( See My Comment in the October 25, 2022 post in Dr. Smith’s ECG Blog ). Look at V1.
That volatile course included Atrialflutter with RVR: == MY Comment , by K EN G RAUER, MD ( 7/11 /2023 ): == It's always rewarding to get "a Save!" — as in today's case, in which this 40-something year old patient with persistent VFib, followed by an extended complicated course — ultimately survived with intact neurologic status!
Sinus tach will rarely remain exactly constant, while PSVT or flutter will always have the same re-entrant rate 2. See many cases with use of Lewis Leads on this blog: Case continued The providers jumped to conclusions and gave adenosine. Try Lewis Leads. This is using the Monitor leads, not the 12-lead electrodes!
male with pertinent past medical history including Atrial fibrillation, atrialflutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia.
Re-entrant tachycardias (atrialflutter, PSVT, AVRT, VT) have constant regular heart rates, whereas sinus tachycardia will usually gradually change rate with differing conditions (for instance, after infusion of fluid and BP increase, sinus tach rate might decrease from 130 to 125, for instance). So there is a re-entrant rhythm.
So this is an extremely slow atrialflutter with 2:1 conduction. Atrial rate 146, ventricular rate 73. I suspect that the amyloid slows the conduction of the atrialflutter. It turned out that he had a history of slow atrialflutter. It turns out that this patient has cardiac amyloidosis.
If it is atrial fibrillation with a rapid ventricular response without a secondary cause, what is the intervention? and runs through 10 cases to elucidate the nuances of atrial fibrillation management on this ECG Cases blog. The post ECG Cases 28 Approach to Atrial Fibrillation appeared first on Emergency Medicine Cases.
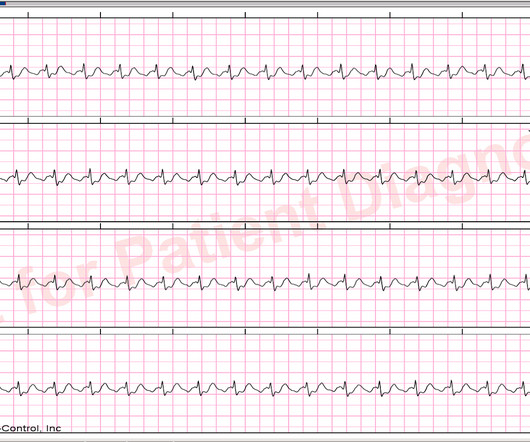
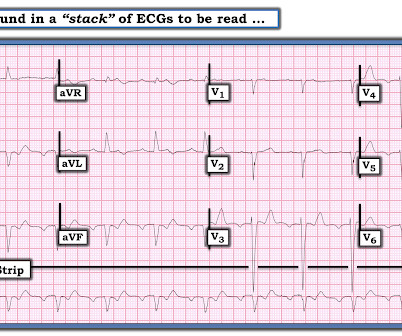
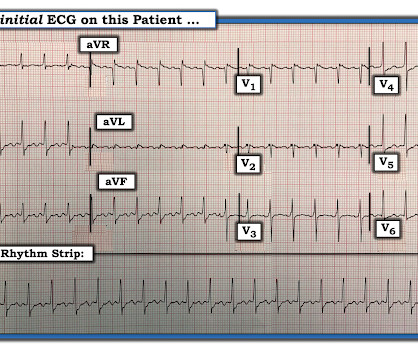
M y A pproach to this R hythm : I reviewed the basics for rhythm interpretation in the October 16, 2019 Case from Dr. Smith’s ECG Blog. In such cases — use of an alternative lead system, such as a L ewis L ead may enhance atrial activity and facilitate rhythm determination. Figure-1: The initial ECG in this case ( See text ).
The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrialflutter with regular conduction. There are no P waves preceding the QRS complexes, and no clear flutter waves. We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia.
The rhythm is 2:1 atrialflutter. The flutter waves can conceal or mimic ischemic repolarization findings, but here I don't see any obvious findings of OMI or subendocardial ischemia. The bedside echo showed a large RV (Does this mean there is a pulmonary embolism as the etiology?) Here is his triage ECG: What do you think?
Are the wide complexes due to a supraventricular rhythm (AVNRT or Atrialflutter or atrial fib) with aberrancy? The rhythm alternates between a wide complex (first 4 beats, and beats 16-28) and narrow complex (beats 5-15). There are no P-waves. Or are they due to ventricular tachycardia (VT).
M Y A NSWER: The issue of whether C omputerized E CG I nterpretations are “at fault” for an inaccurate ECG diagnosis has been addressed numerous times on this blog. M Y A NSWER: In my experience, MAT is the 2nd-most commonly overlooked cardiac arrhythmia ( surpassed only by AtrialFlutter ).
The Differential Diagnosis is: SVT with aberrancy(#) [AVNRT vs. WPW (also called AVRT*)] Atrialflutter with 1:1 conduction, with aberrancy VT coming from the anterior fascicle ( fascicular VT )@ *AVRT = AV Reciprocating Tachycardia (Tachycardic loop that uses both the AV node and an accessory pathway.
Atrialflutter with 2:1 conduction. The atrialflutter rate is approximately 200 bpm, with 2:1 AV conduction resulting in ventricular rate almost exactly 100 bpm. Further history revealed she had new onset atrialflutter soon after her aortic surgery, and was put on flecainide approximately 1 month ago.
2 months later, he presented in pulmonary edema with atrialflutter and formal echo had EF 20% Why did this happen? Regional wall motion abnormality-posterior. Regional wall motion abnormality-lateral. Decreased left ventricular systolic performance moderate.
It is atrialflutter with 2:1 conduction. There are clear flutter waves in lead II across the bottom. In V1, there are upright waves that appear to be P-waves but are not: they are atrial waves and it is typical for atrialflutter waves to be upright in V1, whereas sinus P-waves are biphasic in V1.
The rhythm differential for narrow, regular, and tachycardic is sinus rhythm, SVT (encompassing AVNRT, AVRT, atrial tach, etc), and atrialflutter (another supraventricular rhythm which is usually considered separately from SVTs). Therefore this patient is either in some form of SVT or atrialflutter. If so, why?
There is atrial activity before every QRS, but that activity has negative polarity, so it is not sinus rhythm. There are clearly no flutter waves, so it is not atrialflutter (a "macro-reentrant" atrial tachycardia) Is it AVNRT originating at the superior pole of the AV node, resulting in a retrograde P-wave before the QRS?
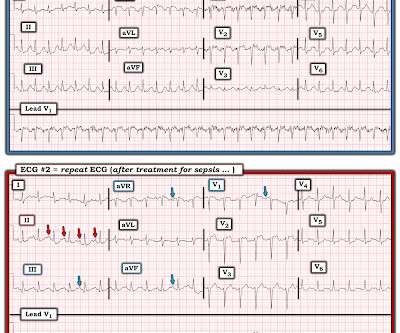
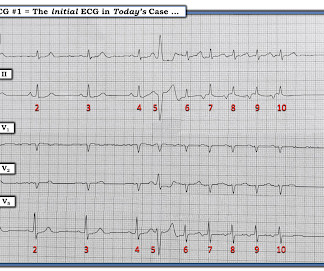
LAFB, atrialflutter, anterolateral STEMI(+) OMI. Fragmentation and artifact ( and possibly already in the inferior leads, the AtrialFlutter pointed out by Dr. Meyers that became obvious in the repeat ECG ) combine to make assessment of ST-T wave changes on many of the leads in ECG #1 difficult.
They are not mysteries: If you actually look at those patients (all listed in the Appendix), they all have serious problems while in the ED: atrial fib, atrialflutter, SOB, Chest pain, generalized weakness, SVT diagnosed by medics, upper GI bleeding 2 days prior, profound bradycardia in the ED, and more.
Before each of these WCT episodes the atrial rate decreased. Whenever the atrial rate remained over 190/minute there was always 2:1 or 3:2 conduction of atrialflutter. I went through all the telemetry recordings and found that the patient had a number of short WCT episodes.
Cardioversion is most beneficial for reentrant arrhythmias ( e.g. VT, atrialflutter, AVNRT, atrial fibrillation) because it terminates the reentry circuit. Atrial tachycardia can occasionally be due to reentry, but reentrant circuits usually have a more stable cycle length without so much beat to beat variability.
The intricacies of the different classes of antiarrhythmics and their mechanism of action extend beyond the scope of this blog. I list below links to other cases of idiopathic VT from Dr Smith's ECG blog. Try a different kind of antiarrhythmic. This is what was done in today's case.
Possible but, again, the QRS morphology is atypical 3) AtrialFlutter with 2:1 conduction and "aberrancy". I do not see flutter wave baseline, and again the QRS morphology is not typical for a supraventricular rhythm. See this case, for example: A Relatively Narrow Complex Tachycardia at a Rate of 180.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content