This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Atrialflutter (AFL) and atrial fibrillation (AF) are believed to carry the same risk of systemic thromboembolism however there is paucity of data concerning such risk in patients with AFL in comparison to AF.
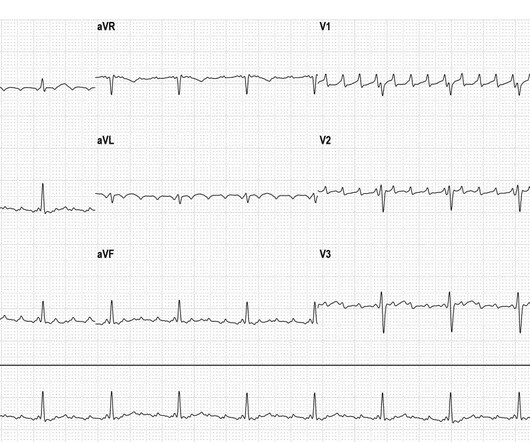
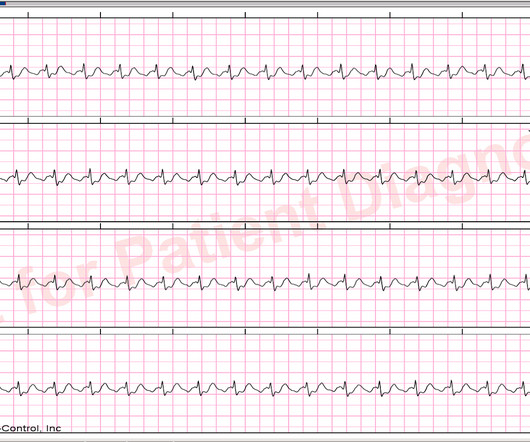
Why is this left atrial atypical atrialflutter ( ECG 1 )? Atrial fibrillation can be excluded because nice flutter waves (all look the same) can be clearly identified. The flutter waves are positive in V1 ( ECG 2 ). The flutter waves are positive in V1 ( ECG 2 ).
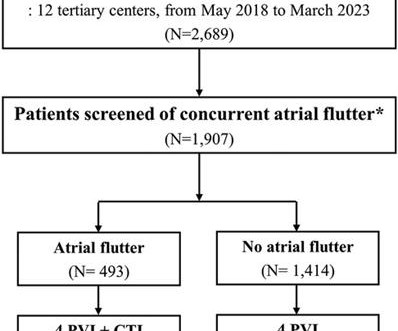
Typical atrialflutter commonly occurs in patients with atrial fibrillation (AF). Limited information exists regarding the effects of concurrent atrialflutter on the long-term outcomes of rhythm control. Patients who were screened for typical atrialflutter were included in the analysis ( n = 1,907).
Atrialflutter and atrial fibrillation are 2 different cardiac arrhythmias, but occur frequently side by side in the same patient. Here is an example of how atrialflutter degenerataes into atrial fibrillation.
a medical technology company focused on transforming cardiac care through the power of personalized insights, today announced new study data demonstrating that HeartBeam AI combined with vectorcardiography (VCG) outperformed an expert panel of heart rhythm cardiologists in detecting atrialflutter. The data was presented by Joshua M.
A 24-hour 12-lead ECG revealed sinus rhythm, frequent atrial premature beats, paroxysmal atrialflutter with an atrialflutter burden of 9.37% and no paroxysmal ST-T abnormalities. Observations revealed a normal temperature of 36.5°C °C and a normal blood pressure of 123/83 mm Hg.
In the study, HeartBeam AI with VCG demonstrated a 28% improvement over single-lead ECG in the detection of atrialflutter cases (sensitivity of 91.0% for single-lead ECG) without sacrificing the ability to identify those individuals without atrialflutter (specificity of 98.7% for VCG vs. 71.2% for VCG vs. 96.9%
Atrialflutter (AFL) in nave hearts is predominantly typical peritricuspid AFL; atypical AFL is seen post cardiac surgery or atrial fibrillation (AF) ablation.
While atrial arrhythmias are frequently associated with SSS, we hypothesized that atrialflutter (AFL) would strongly predict SSS given shared relationships with right atrial, and particularly crista terminalis, fibrosis.
Heart failure (HF) readmission rates remain a concern in patients with lone typical atrialflutter (AFL) and HF, even following cavo-tricuspid isthmus (CTI) ablation.
Cavotricuspid isthmus (CTI) ablation for patients presenting with typical atrialflutter (AFL) is a highly effective intervention, however these patients are at risk for developing atrial fibrillation (AF).
Atypical atrialflutter (AtFL) and atrial fibrillation (AF) share similar clinical presentations but may differ in underlying substrates and clinical progression.
We present a case of successful PFA of an atrialflutter in a patient with d-TGA. There is a paucity of literature regarding PFA in complex congenital heart disease.
While atrial arrhythmias are frequently associated with SSS, we hypothesized that atrialflutter (AFL) would strongly predict SSS given shared relationships with right atrial, and particularly crista terminalis, fibrosis.
Little is known about the treatment of atypical atrialflutter that occurs after PFA of AF. Pulsed field ablation (PFA) has emerged as an innovative new ablation strategy for the treatment of AF.
Pulsed-field ablation (PFA) has the potential to improve safety and efficacy in atrialflutter (AFL) ablation, yet its clinical outcomes and procedural characteristics remain underexplored in real world practice.
Given the pentaspline catheter design of the FARAPULSE system, applications of PFA may inadvertently result in narrow channels of slow conduction along the posterior wall between lesion sets, creating a substrate for left atrialflutter.
BackgroundTypical isthmus-dependent atrialflutter (AFL) is traditionally treated through radiofrequency (RF) ablation to create a bidirectional conduction block across the cavo-tricuspid isthmus (CTI) in the right atrium.
Atrialflutter/atrial tachycardia (AFL/AT) detection performance in insertable cardiac monitors (ICM) remains a challenge due to inappropriate detections.
Traumatic brain injury (TBI) is associated with a variety of adverse long-term outcomes and increases sympathetic nervous system activation which could increase the risk of arrhythmias including atrial fibrillation or atrialflutter (AF/AFL).
Idiopathic atypical (non-cavotricupid isthmus [CTI]-dependent) atrialflutter (IAAFL) may be seen in patients without structural heart disease and without previous cardiac surgery or ablation.
Atypical AtrialFlutter (AAFL) prevalence is increasing due to the escalating Atrial Fibrillation (AF) ablations and cardiac surgeries. We wanted to explore the outcome of the AAFL ablation, considering the recent changes in mapping and ablation.
ABSTRACT Background Atrial fibrillation and atrialflutter are relatively rare in young people and the incidence of thromboembolic complications is unknown. These issues contribute to the limited utility of present guidelines regarding anticoagulation in this population.
Cavo-tricuspid isthmus (CTI) dependent atrialflutter (AFL) is one of the most common atrial arrhythmias involving the right atrium (RA). Radiofrequency catheter ablation has been widely used as a therapy of choice and it is curative.
A significant proportion of patients with isolated atrialflutter (AFL) will develop atrial fibrillation (AF) following cavotricuspid isthmus (CTI) ablation.
ABSTRACT Atrialflutter (AFL), defined as macro-re-entrant atrial tachycardia, is associated with debilitating symptoms, stroke, heart failure, and increased mortality. Atypical AFL is a heterogenous group of re-entrant atrial tachycardias that most commonly occur in patients with prior heart surgery or catheter ablation.
Image-based patient-specific computational models have recently emerged as a tool to guide atypical atrialflutter (AAF) ablation. However, little is known about the sensitivity of these models to the selection of parameters.
The competing risk of non-stroke mortality may limit the potential benefit of stroke prophylaxis therapy in patients with atrial fibrillation and/or atrialflutter (AF).
Concerns about the safety of coronavirus disease (COVID-19) vaccines in patients with atrial fibrillation/atrialflutter (AF/AFL) have arisen due to reports of an association between thromboembolic events and COVID-19 vaccination.
However, there is a need to deliver flexible lesions for atrialflutter (AFL) and non-PV ablations. Single-shot pulsed field ablation (PFA) catheters for pulmonary vein isolation are being studied. A 7Fr PFA catheter (PFLinear, EnChannel Medical) capable of delivering both focal and linear ablations has been developed.
It is unclear how deep learning applied to VCG compares to physicians (EPs) for atrialflutter (AFL) detection. The representation of ECG vectors in X, Y, and Z axes in a vectorcardiogram (VCG) has shown diagnostic promise beyond single lead ECG (SL) analysis, with implications for novel ECG acquisition technologies.
If a wide complex tachycardia occurs, the probability is very high that it is a ventricular tachycardia (approx. 80%, in patients with a previous myocardial infarction (.) Here we see a broad complex tachycardia that looks like an RBBB + LAFB, which is regular. In this constellation, 3 causes must be considered: 1.
Head CT scans showed hypoattenuating areas indicative of cerebral infarction, chest CT suggested possible air accumulation in the left atrial region. ECG findings were consistent with atrialflutter, myocardial infarction, and incomplete right bundle branch block.
Wild-type transthyretin amyloid cardiomyopathy (ATTRwt-CM) is often accompanied by atrial fibrillation (AF), atrialflutter (AFL), and atrial tachycardia (AT), which are difficult to control because beta-blockers and antiarrhythmic drugs can worsen heart failure (HF).
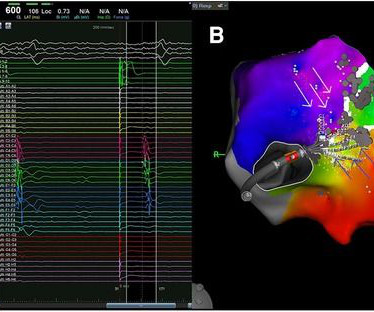
Reversible pulsed field ablation (PFREV) can temporarily block conduction and may emerge as a novel clinical mapping tool to accurately identify critical isthmuses before creating permanent lesions.
Abstract Introduction Cavo-tricuspid isthmus (CTI) dependent atrialflutter (AFL) is one of the most common atrial arrhythmias involving the right atrium (RA) for which radiofrequency catheter ablation has been widely used as a therapy of choice.
The positive F wave in lead V1 changed during entrainment from the right atrial appendage (RAA) during typical atrialflutter (AFL). Abstract Introduction Typical atrialflutter (AFL) is a macroreentrant tachycardia in which intracardiac conduction rotates counterclockwise around the tricuspid annulus.
A fully upright P-wave is typical atrial activity of atrialflutter as seen in V1. See these example cases of upright P-waves: Case Continued Thus, I was all but certain that this was atrialflutter.
If it is slow Atrialflutter with 1:1 conduction, it should slow the conduction and reveal the flutter waves. This is the exact rate one expects with slow atrialflutter and it is why slow atrialflutter can be so dangerous: it conducts 1:1, with fast ventricular rates. Rate 120, flutter rate 240.
- PSVT (which includes AVNRT and orthodromic AV reciprocating tachycardia) [AVRT uses an accessory pathway, a "bypass tract" and thus is seen in WPW; about 30% of PSVT is orthodromic AVRT] - AtrialFlutter with 1:1 conduction. If you look closely at lead II across the bottom, it appears there are flutter waves. Which is it?
Reversible pulsed field ablation (PFREV) can transiently interrupt cardiomyocyte conduction, offering a promising mapping tool that could precisely identify critical isthmuses within tachycardia circuits before creating permanent lesions.
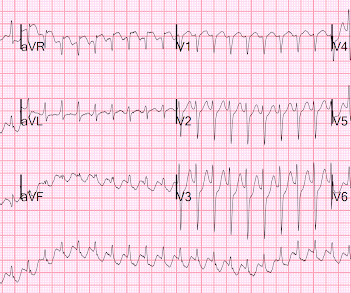
There is the appearance of STE in inferior leads II, III, and aVF (with STD in aVR), but this is entirely due to flutter waves which are only seen in those leads. Also, the atrialflutter in this case is relatively slow like in many other cases we've shown. AtrialFlutter with Inferior STEMI? Is this inferor STEMI?
Primary endpoint was the incidence of patients with new onset supraventricular arrhythmia (AF, atrialflutter or any supraventricular tachycardia) lasting >30s, post PFO closure.ResultsA total of 59 patients met the inclusion criteria.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content