This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The increased use of radiofrequency ablation (RFA) for atrialfibrillation (AF) has led to a rise in cases of pulmonary vein stenosis or occlusion (PVS/O) as a complication. While this occurrence was once rare, the growing number of patients undergoing this procedure has made it more prevalent.
When atrialfibrillation (AF) begins, it can start with a single focus, degenerating to multiple wavelets, and it spreads throughout the entire surface area of both atria. A fibrillatory wave that occurs at a rate of more than 600 beats per minute can cause fatigue in the long run, leading to atrial dilation.
Atrialfibrillation (AF) and coronary artery disease are frequently associated and, when so, lead to a grim prognosis. The clinical impact of correct assessment of coronary artery stenosis in AF is especially high, due to the antithrombotic therapy imposed by both AF and coronary stenting.
BackgroundAortic valve calcium score is associated with hemodynamic severity of aortic stenosis. years, 47% of patients were women, 50% had coronary artery disease, 40% had atrialfibrillation, 47% had prior cardiac surgery, and 33% had prior chest radiation. Median patient age was 66.9±11.2 mm Hg on echocardiography and 8.5±4
Titled "Real-world Data Affirms Safety and Effectiveness of Low/Zero Fluoroscopy AtrialFibrillation Ablation," the study was presented as a late-breaker at the 29th Annual International AF Symposium. 1 These included one pseudoaneurysm, one PV stenosis and one hematoma.1 Epidemiology of AtrialFibrillation in the 21st Century.
Cryoablation for atrialfibrillation is a widely used technique for pulmonary vein isolation. Known complications associated with cryoablation include tamponade, phrenic nerve injury, stroke, pulmonary embolism, pulmonary vein stenosis, and atrioesophageal fistulas.
intermittent) atrialfibrillation (AF) and is a unique new alternative to standard-of-care thermal ablation treatment. intermittent) atrialfibrillation (AF) and is a unique new alternative to standard-of-care thermal ablation treatment. said Nick Spadea-Anello, president, Electrophysiology, Boston Scientific.
Case summary An 85-year-old woman suffering from long-standing atrialfibrillation and severe symptomatic aortic stenosis underwent SE TAVI (26 mm Evolut™ R®, Medtronic Inc.,
Percutaneous balloon mitral valvotomy (PBMV) is a good and preferred therapy choice over surgical commissurotomy for patients with rheumatic mitral stenosis (MS).
The left atrial appendage (LAA) is a potential trigger for atrialfibrillation (AF) and emerging evidence supports the role of electrically isolating the LAA in select patients. However, concerns regarding complications of such a procedure remain unclear.
Objective To investigate the impact of prior coronary artery bypass grafting (CABG) and coronary lesion complexity on transcatheter aortic valve replacement (TAVR) outcomes for aortic stenosis. Conclusion Prior CABG may positively affect mid-term TAVR outcomes for aortic stenosis compared with no CAD when adjusted for other comorbidities.
Publication date: 15 January 2024 Source: The American Journal of Cardiology, Volume 211 Author(s): Heikki J. Niemi, Satu Suihko, Minna Kylmälä, Helena Rajala, Suvi Syväranta, Sari Kivistö, Jyri Lommi
Background: Atrialfibrillation (AF) is common in patients undergoing transcatheter aortic valve replacement (TAVR) and is associated with increased risk of bleeding and stroke. Conclusions: Concomitant WATCHMAN LAAO and TAVR is noninferior to TAVR with medical therapy in severe aortic stenosis patients with AF.
Background:Myocardial infarction with nonobstructive coronary artery disease (MINOCA) is a special syndrome with clear evidence of myocardial ischemia, but no clear stenosis of coronary artery imaging sign. The pericoronary fat attenuation index (FAI) could reflect the local coronary inflammation as a novel imaging marker.
Examples of cardio embolic stroke etiology include: 1. AtrialFibrillation 2. Cardiomyopathy with mural thrombus 3. Patent Foramen Ovale 4. Severe calcific Aortic (valve) Stenosis 5. Mechanical prosthetic valve Severe carotid artery stenosis is also implicated in embolic stroke. We do have the ECG.
001) and postoperative atrialfibrillation occurred less frequently (p = .044) This was a retrospective, single-center observational study. The patients were divided into two groups: the hemisternotomy group (n = 100) and the right anterior thoracotomy group (n = 74).ResultsThe ResultsThe overall in-hospital mortality was 1,7%.
Pulsed Field Ablation is a relatively new modality for treatment of atrialfibrillation. In conventional ablation for atrialfibrillation, either heating of tissue is produced by radiofrequency application or freezing of tissues by cryoablation. N Engl J Med. 2023 Nov 2;389(18):1660-1671. doi: 10.1056/NEJMoa2307291.
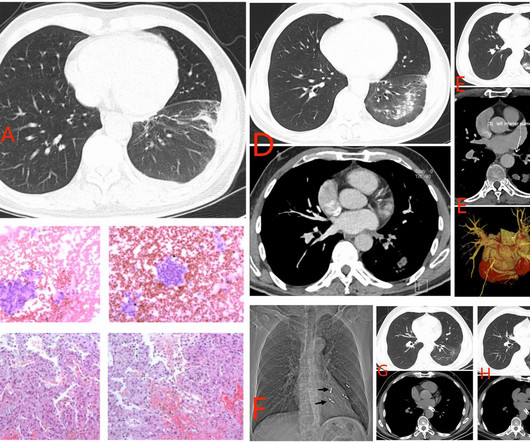
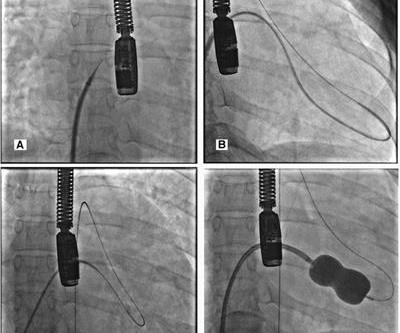
Method and Results A 54-year-old man with long history of atrialfibrillations developed PVS secondary to multiple radiofrequency ablation procedures. The stenosis was treated with a stent. Balloon angioplasty seems to be the widely preferred treatment of choice.
Pulsed field ablation (PFA) is a new treatment for atrialfibrillation (AF), and its selective ablation characteristics give it a significant advantage in treatment. There were no recurrences, PV stenosis, or other serious adverse events during the 12 months follow-up.
Here was his initial ED ECG: There is atrialfibrillation with a rapid ventricular response. ST depression is common BOTH after resuscitation from cardiac arrest and during atrial fib with RVR. The estimated left ventricular ejection fraction is 58 % Aortic stenosis, mild, 9.0 A middle-aged male had a V Fib arrest.
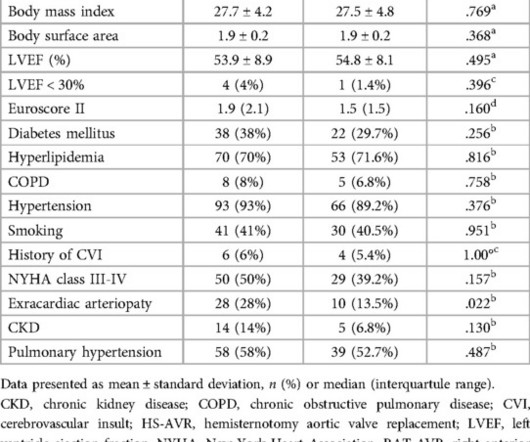
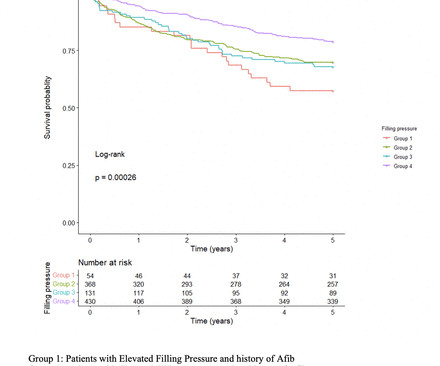
Background Increase in left ventricular filling pressure (FP) and diastolic dysfunction are established consequences of progressive aortic stenosis (AS). years and were more likely to be males (62%), diabetic (41% vs 35%, p=0.046), and have a higher prevalence of atrialfibrillation (Afib) (53% vs 39%, p<0.001).
BackgroundChronic inflammatory disease (CID) accelerates atherosclerosis and the development of aortic stenosis. Patients with CID were predominantly female (60% versus 44%,P=0.002) and more often had pulmonary disorders (21% versus 13%,P=0.046) and atrialfibrillation (32% versus 20%,P=0.003). and 1.62, respectively).
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrialfibrillation, pacemaker (placed 1 month earlier), LBBB. This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System.
However, CTA head and neck 4 days later demonstrated 90 percent stenosis of the mid left V2 at the C3‐4 level and a 75‐90 percent stenosis of the left mid V2 segment at the C5‐6 level (hard and soft plaque in these areas). He also had moderate stenosis of the right V4 segment.
Transcatheter Mitral Valve Repair is Cost-Effective in Heart Failure Patients TAVR Expected to See Rapid Growth in Next 5 years FDA Clears Abbott Amplatzer Amulet LAA Occluder to Reduce Stroke in People With AtrialFibrillation Portico TAVR System Found Safe and Effective for High-Risk Surgical Patients Portico TAVR System Reduces Severe (..)
24 will focus on the following three current guideline updates: American College of Cardiology (ACC)/American Heart Association (AHA) Guidelines 2023 AtrialFibrillation Guideline - Pharmacology II: Strokes vs. Bleeds, What Do the Guidelines Tell Us About Practical Management in A-fib? The Guidelines Sessions at ACC.24
ICAD group was defined as persistent occlusion or residual stenosis at the initial occlusion site. ICAD group had lower atrialfibrillation frequency, lower BNP levels, more M1 occlusions, and fewer M2 occlusions compared to the Embolic group. Successful recanalization was defined as Thrombolysis in Cerebral Ischemia score ≥2b.
A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity. The aortic valve in this example also had critical stenosis by Doppler The patient continued to be hemodynamically unstable with poor cardiac output and very high LV filling pressures.
Objective This study compared procedural and outcome data for PFA-PVI to VHPSD-PVI in patients with paroxysmal or persistent atrialfibrillation (PAF/persAF). One clinically nonsignificant PV stenosis occurred in the VHPSD group. Data comparing PFA to VHPSD-PVI is lacking.
million suffer from long-term complications including heart failure, atrialfibrillation, stroke and infective endocarditis. Although largely preventable, 33.4 RHD is the most commonly acquired heart disease for people under 25 years old and over 1.2
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrialfibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. Anything more on history? Left main?
The rhythm is nearly regular, but there are no P-waves (it is too regular to be atrialfibrillation). Also, anterior MI could result from 1) ACS, but also from 2) severe ischemia due to combination of a hemodynamically significant LAD stenosis + severe hypotension during cardiac arrest. at the time of the ECG. Mg was 1.6.
During its Annual Conference, HRS 2024, the Heart Rhythm Society (HRS) announced findings from three new studies demonstrating the safety and efficacy of pulsed field ablation (PFA), a nonthermal ablation treatment for patients with atrialfibrillation (AF). See full findings from the FARADISE, admIRE Study, and Advent Trial here.
The primary safety endpoint was incidence of early onset (within seven days) primary adverse events; atrio-esophageal fistula (within 90 days); cardiac tamponade or perforation (within 30 days); and PV stenosis (within 12 months). Global epidemiology of atrialfibrillation: An increasing epidemic and public health challenge.
Here I annotate it: This shows 100% occluded circumflex (red arrow) and a 90% stenosis of the LAD (Yellow arrow). The LAD was thought to be not thrombotic, but a chronic tight stenosis. ECG from 2 days later: AtrialFibrillation now. Inverted Reperfusion T-waves inferior Learning Points: 1.
ABSTRACT Introduction The safety and efficacy of paroxysmal atrialfibrillation (PAF) ablation with the HELIOSTAR multielectrode radiofrequency (RF) balloon catheter have been demonstrated in European studies; data from elsewhere are lacking. Central Illustration. Image is courtesy of Biosense Webster, Inc., All rights reserved.
Background:Patients with atrialfibrillation were excluded from clinical trials evaluating carotid artery stent(CAS) or carotid endarterectomy (CEA).We We used the ICD-10 to identify patients hospitalized with diagnosis of stroke, TIA, or retinal ischemia with stenosis of carotid artery who underwent CAS or CEA. versus 18.8%
BACKGROUND:Pulsed field ablation (PFA) is a promising treatment for atrialfibrillation. Patients with paroxysmal or persistent atrialfibrillation underwent pulmonary vein (PV) isolation under deep sedation or general anesthesia and returned for remapping at 90 days to evaluate chronic durability. paroxysmal, and 58.5%
Objective Patients with low-flow, low-gradient aortic stenosis (LFLG AS) and reduced left ventricular ejection fraction (LVEF) are known to suffer from poor prognosis after transcatheter aortic valve implantation (TAVI). This study aimed to develop a simple score system for risk prediction in this vulnerable subset of patients.
BACKGROUND:Current guidelines recommend surgical aortic valve replacement (SAVR) for patients with severe aortic stenosis and unfavorable iliofemoral access. Acute kidney injury stages 2 to 4, bleeding events, and new-onset atrialfibrillation occurred more often in the SAVR group during the hospital period (P<0.001).
Research is also underway into algorithms for the diagnosis of Aortic Stenosis and Myocarditis and should be ready for commercialization in the next 18 – 36 months. In late 2023, HeartSciences announced a partnership with the Icahn School of Medicine at Mount Sinai to commercialize the latter’s extensive ECG data and algorithm library.
Background:Previous reports have established a relationship between asymptomatic high-grade carotid artery stenosis (CAS) and impaired cognition. Conclusion:Cardiac disease is common among patients with asymptomatic high-grade carotid stenosis and may have a synergistic effect on impairments in memory in a manner not mediated by stroke.
VHD incidence was determined using International Classification of Disease-10 codes for aortic stenosis (AS), aortic regurgitation (AR), mitral stenosis, mitral regurgitation (MR) and mitral valve prolapse. Clinical correlates of VHD included demographics, coronary artery disease, heart failure and atrialfibrillation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content