This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
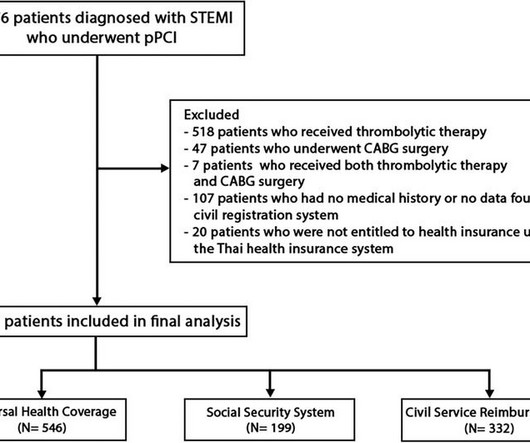
BackgroundIn Thailand, access to specific pharmaceuticals and medical devices for ST-elevation myocardial infarction (STEMI) patients is restricted within certain healthcare systems, leading to inequalities in the quality of medical care among different healthcare systems.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrialfibrillation, pacemaker (placed 1 month earlier), LBBB. Most large STEMI have peak troponin I in the 20.0 She reports associated SOB but no dizziness or LOC.
It's a very "fun" ECG, with initial ectopic atrial tachycardia (negative P waves in inferior leads conducting 1:1 with the QRSs), followed by spontaneous resolution to sinus rhythm. In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. No use of drugs, stimulants, etc.
Here was his initial ED ECG: There is atrialfibrillation with a rapid ventricular response. ST depression is common BOTH after resuscitation from cardiac arrest and during atrial fib with RVR. We found that 38% of out of hospital ventricular fibrillation was due to STEMI. A middle-aged male had a V Fib arrest.
One might think this represents acute STEMI, or Bundle branch block with discordant ST segments and suspicously concordant T-waves. Upon arrival to the ED, he had the following 12-lead ECG: There is striking ST segment elevation in V1 and V2, with ST depression in V3-V6 as well as I, II, and aVF. There is also a wide QRS.
The medical care providers ascribed the patient's chest pain to new onset atrialfibrillation with rapid ventricular response after having viewed the ECG. The presentation ECG does show atrialfibrillation. No further episodes of atrialfibrillation occurred during monitoring. The first ECG is shown below.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrialfibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. J Electrocardiol 2013;46:240-8 2.
What is the atrial activity? Or is it atrialfibrillation with complete AV block and junctional escape? There is an obvious inferior posterior STEMI(+) OMI. Results Of 149 patients with inferior STEMI , 43 (29%) had RVMI and 106 (71%) did not. Here is his ED ECG: There is bradycardia with a junctional escape.
The rhythm is nearly regular, but there are no P-waves (it is too regular to be atrialfibrillation). The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The patient had a combined respiratory and metabolic acidosis (as we commonly find in those with prolonged arrest), and a K of 4.1,
In this ECG Cases blog Dr. Jesse McLaren guides us through 10 cases, driving home the points that sepsis is a common cause of rapid Afib and diffuse ST depression with reciprocal ST elevation in aVR, myo/pericarditis is a diagnosis of exclusion, endocarditis or lyme carditis can cause AV block, PE can cause low grade fever and ECG signs of acute RV (..)
On this month's EM Quick Hits podcast David Carr on differential diagnosis of normal unenhanced CT renal colic, Leeor Sommer on recognition and management of perichondritis and auricular abscess, Suzanne Schuh on IV magnesium sulphate for pediatric asthma, Jess McLaren on Occlusion MI ECG interpretation requiring cath lab activation and Justin Morgenstern (..)
edits by Meyers A woman in her 60s with a history of chronic atrialfibrillation on Eliquis, ESRD on hemodialysis, type-II diabetes mellitus, prior CVA, hypertension, and hyperlipidemia presented to the emergency department with multiple complaints after missing dialysis. Is this inferor STEMI? Christmas Eve Special Gift!!
He was brought to the critical care area where these rhythms were seen on the monitor: Wide complex tachycardia with no apparent P-waves, and very irregular Consistent with atrialfibrillation with aberrancy A Regular wide complex tachycardia. Looks like atrialfibrillation. LV Aneurysm? Would you give Thrombolytics?
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. Look at the aortic outflow tract. What do you see? Answer below in the still shot.
This can only be due to STEMI. ECG from 2 days later: AtrialFibrillation now. However, cardiogenic shock usually takes some time to develop, so it is probably subacute." Then I was told that the troponin I returned at greater than 50,000 ng/L. I said "activate the cath lab." Circumflex occlusion may have minimal ECG findings.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? There is atrialfibrillation. to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 The corrected QT interval is extremely long, about 500 ms. The QT is much shorter still.
Here is his ECG: There is atrialfibrillation at a rate of 95. Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Exact pain history was difficult to ascertain. There was some SOB.
Description There is atrialfibrillation at a rate of 95. Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. He had walked into the ED (did not use EMS).
ACS QID 75345 In 2017, the New England Journal of Medicine published the results of the Dual Antithrombotic Therapy with Dabigatran after PCI in AtrialFibrillation (RE-DUAL PCI) trial. Explanation: The EKG illustrates an inferior STEMI. Severe mitral stenosis C. Hyperdynamic ventricle D. Acute mitral regurgitation E.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. Chart review confirmed that he had been started on flecainide for atrialfibrillation. Is that an obvious STEMI underneath that rhythm? Is this inferor STEMI?
So this is a typical Brugada syndrome ECG, which can be easily mistaken for an acute myocardial infarction with ST elevation in anterior leads may be taken as STEMI if the person presents with chest pain for some other reason. Of course, the commonest sustained arrhythmia in general population is atrialfibrillation.
The rhythm is atrialfibrillation. Initial ROSC was obtained, during which this ECG was obtained: What do you think? Meyers interpretation: This is a complicated interpretation made even more so by the fact that it is immediately post ROSC. The QRS complex is within normal limits.
underlying atrialfibrillation or atrial inactivity). And, in cases like the elderly patient with new-onset chest pain presented here — definitive diagnosis of acute STEMI is sometimes deceptively easy. BOTTOM LINE: Despite cardiac pacing — ECG #2 is diagnostic of a very large acute anterior STEMI.
The computer called this Acute STEMI What do you think? STEMI never has a very short QT. There is Bazett, Fridericia, Hodges, Framingham and Rautaharju -- see here at mdcalc: [link] If the ST Elevation here were due to STEMI, it would be an LAD Occlusion.
Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. An EKG from a year prior was available for comparison: The ED physician noted Initial EKG here read by the computer as a STEMI, however, there is a very poor baseline and a lot of artifact. See reference and discussion below.
ECG met STEMI criteria and was labeled STEMI by computer interpretation. J waves can also be induced by Occlusion MI (5), STEMI mimics including takotsubo and myocarditis complicated by ventricular arrhythmias (6, 7), and subarachnoid hemorrhage with VF (8). Take home : Not all STEs are STEMIs or OMIs. What do you think?
2:34 PM, following right heart catheterization She then went into atrialfibrillation with complete heart block and junctional escape rhythm prompting placement of transvenous pacemaker. There was indication of parasympathetic overdrive ( the acute inferior STEMI with profound bradycardia and junctional escape ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content