This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
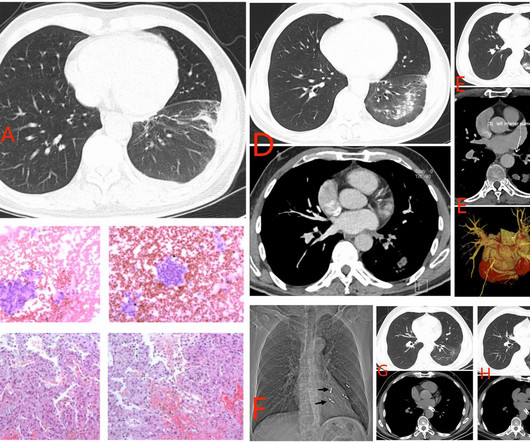
The increased use of radiofrequency ablation (RFA) for atrialfibrillation (AF) has led to a rise in cases of pulmonary vein stenosis or occlusion (PVS/O) as a complication. The actual frequency of pulmonary vein (PV) occlusion remains a topic of debate.
In particular, the study showed superiority in the percentage of patients that achieved freedom from atrialfibrillation (AF) with or without anti-arrhythmic drugs at 12 months after a tailored cardiac ablation guided by AI in combination with PVI when compared to PVI alone. tim.hodson Fri, 02/14/2025 - 09:57 Feb. adult population.
Atrialfibrillation is the most prevalent arrhythmia with a lifetime risk of nearly 30%. Pulmonary vein isolation (PVI) is the most effective treatment for rhythm control. It can be associated with reduced quality of life and complications such as heart failure and stroke.
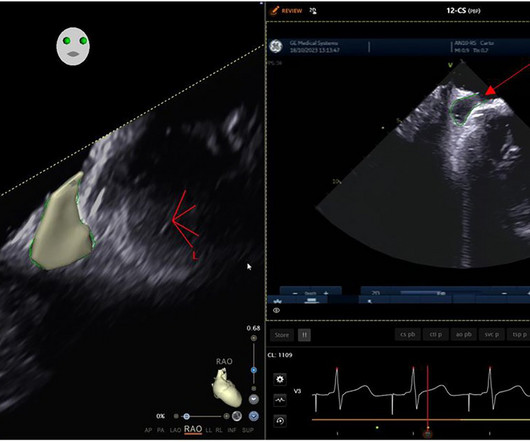
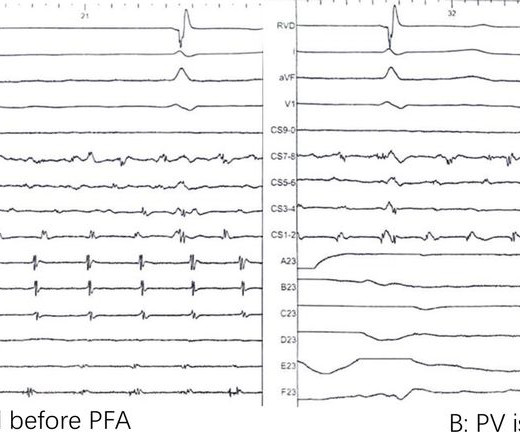
Objective Pulsed-field ablation (PFA) is a new technology of catheter ablation for atrialfibrillation (AF). After a successful transseptal puncture, the PFA catheter (CardiPulse) was delivered to the different pulmonary veins sequentially for standard PFA, and the pulmonary vein electrical isolation (PVI) was observed in real-time.
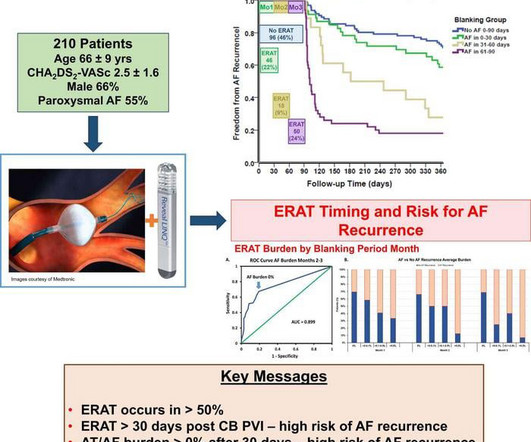
Based on continuous monitoring of early recurrence of atrial tachyarrhythmia immediately after patients have undergone atrialfibrillation ablation, Musat et al. recommend shortening the blanking period from three months to one. also emphasize the importance of continuous monitoring.
Research conducted across 12 hospitals in China has discovered that combining linear ablation with ethanol infusion via the vein of Marshall (EIVOM) alongside pulmonary vein isolation (PVI) significantly improves sinus rhythm maintenance in patients suffering from persistent atrialfibrillation.
Ablation index (AI)-guided pulmonary vein isolation (PVI) has enhanced procedural outcomes for atrialfibrillation (AF).1 1 However, patients with persistent AF present higher recurrence rates due to advanced atrial remodeling,2-3 represented by the left atrial low voltage area (LVA), compared to those with paroxysmal AF.
The VARIPULSE Platform is designed to enable pulmonary vein isolation with the versatility of a catheter loop, a simple generator user interface, and a mapping system that provides an intuitive, reproducible workflow with real-time visualization, contact indicator, and PF tagging mechanisms. Int J Stroke. 2021 Feb;16(2):217-221.
During its Annual Conference, HRS 2024, the Heart Rhythm Society (HRS) announced findings from three new studies demonstrating the safety and efficacy of pulsed field ablation (PFA), a nonthermal ablation treatment for patients with atrialfibrillation (AF). See full findings from the FARADISE, admIRE Study, and Advent Trial here.
Pulmonary vein isolation (PVI) is the cornerstone of interventional treatment for atrialfibrillation (AF). Pulsed-field ablation (PFA), a novel non-thermal modality, was recently introduced and is now available with four different FDA-approved systems from three different manufacturers.
Both atria develop from a combination of the primitive atrium, sinus venous, and pulmonary veins.It When atrialfibrillation (AF) begins, it can start with a single focus, degenerating to multiple wavelets, and it spreads throughout the entire surface area of both atria. The baseline RA dimension is a few mm more than LA.
Pulsed field ablation (PFA) for paroxysmal atrialfibrillation (AF) has been gaining worldwide acceptance due to its efficacy and safety. However, the role of TPI during pulmonary vein (PV) isolation (PVI) is unclear. A variable loop circular catheter (VLCC, VARIPULSE, Biosense Webster, Inc.)
The PulseSelect PFA system was engineered with differentiated safety features and provides rapid, effective pulmonary vein isolation (PVI) through consistent and predictable energy delivery and catheter maneuverability. Mortality trends in patients diagnosed with first atrialfibrillation: a 21-year community-based study.
There have been 2 recent case reports of focal spasm occurring during pulmonary vein isolation (PVI) for atrialfibrillation (AF) using PFA remote from coronary arteries (2,3). Focal coronary spasm is a recognised complication of pulsed field ablation (PFA) delivered within proximity of coronary arteries (1).
Patients in the study will be randomized to undergo pulmonary vein isolation (PVI) and left atrial posterior wall ablation using the FARAPULSE PFA System, or receive AAD treatment, and followed for three years. The randomized AVANT GUARD trial will enroll more than 500 patients diagnosed with persistent AF at up to 75 sites globally.
(MedPage Today) -- LONDON -- Pulmonary vein isolation (PVI) produced real short-term improvements for people with atrialfibrillation (Afib or AF), according to the first sham-controlled trial on the subject. Continuous monitoring by implantable.
The collaboration, according to a written statement issued by the company, aims to address challenges in capturing and analyzing cardiac signals to help physicians enhance patient outcomes for atrialfibrillation procedures. Estimates of current and future incidence and prevalence of atrialfibrillation in the U.S.
Initial findings from feasibility studies on pulsed field ablation (PFA) in the treatment of atrialfibrillation (AF) indicated high rates of efficacy and pulmonary vein (PV) isolation (PVI) durability upon systematic remapping.
The international, multi-center trial will provide clinical evaluation of Cortex's 510(k) cleared Ablamap System with electrographic flow (EGF) and newly released Ablacath Mapping Catheter basket mapping catheter to identify extra-pulmonary vein EGF sources.
male with pertinent past medical history including Atrialfibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Bedside ultrasound showed volume depletion and no pulmonary edema.
Specific cardiovascular diseases, such as acute myocardial infarction, arrhythmias, pulmonary hypertension and pericarditis, were also pointed. Elevated risk of arrhythmias, particularly atrialfibrillation, correlated with occupational silica exposure.
Current guideline indications for intervention in asymptomatic patient are centred on left ventricular dimensions and ejection fraction and may include consideration in atrialfibrillation, pulmonary hypertension and those with left atrial dilatation.
The goal of the SHAM-PVI trial was to compare the clinical efficacy of cryoballoon pulmonary vein isolation (PVI) to a sham procedure in the treatment of symptomatic atrialfibrillation (AF).
Paroxysmal atrialfibrillation is a type of AFib that causes short, intermittent episodes of irregular and rapid heartbeats originating in the atria. Cryoballoon ablation is typically used to treat PAF and involves using a balloon catheter to freeze heart tissue and isolate the pulmonary veins that can cause irregular heartbeats.
Isolation line placed at the pulmonary vein antrum (PVA) area is superior to ostium level in atrialfibrillation (AF) control. However, less is known about the electrophysiological characteristics of PVA.
BackgroundCatheter ablation is frequently used to manage recurrent atrialfibrillation (AF) resistant to drug therapy, with pulmonary vein isolation (PVI) as a key tactic. The reconnection of pulmonary veins was discovered primarily in the anterior region of the right superior PV and the superior portion of the left superior PV.
Cryoablation for atrialfibrillation is a widely used technique for pulmonary vein isolation. Known complications associated with cryoablation include tamponade, phrenic nerve injury, stroke, pulmonary embolism, pulmonary vein stenosis, and atrioesophageal fistulas.
Background: Patients with atrialfibrillation (AF) and concomitant pulmonary hypertension (pHTN) have an increased risk of morbidity and mortality. However, the outcomes of catheter ablation in this cohort are unclear.
(MedPage Today) -- The FDA approved the Farapulse pulsed field ablation (PFA) system for paroxysmal atrialfibrillation (Afib or AF), Boston Scientific announced on Wednesday. The device won an indication for the isolation of pulmonary veins in.
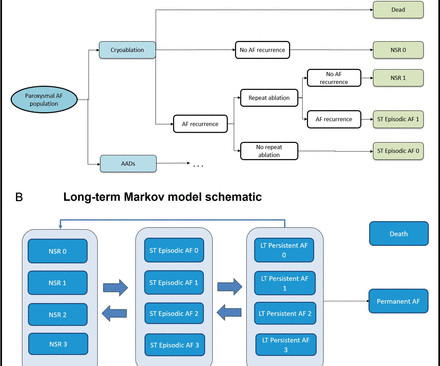
Introduction Three recent randomised controlled trials have demonstrated that pulmonary vein isolation as an initial rhythm control strategy with cryoablation reduces atrial arrhythmia recurrence in patients with symptomatic paroxysmal atrialfibrillation (PAF) compared with antiarrhythmic drug (AAD) therapy.
Abstract Introduction Some previous studies have reported that a first-step ethanol infusion into the vein of Marshall (EIVOM) with touch-up radiofrequency (RF) ablation can facilitate mitral isthmus (MI) block and improves the ablation outcomes in persistent atrialfibrillation (PeAF) patients.
Methods 15 patients with paroxysmal atrialfibrillation were randomized to used fixed-curve, conventional steerable or visualized steerable sheath, and received complete isolation of pulmonary veins. All ablations were the very first procedure performed by 15 ablation apprentices.
At present we do not have any reliable intra-procedural electrophysiologic predictors of long-term success of AF ablation other than pulmonary vein isolation. We evaluated selected intraprocedural pulmonary vein characteristics that may be helpful in future guidance of persistent AF ablation.
Patients with atrialfibrillation (AF) who undergo repeat ablation are more likely to have non pulmonary vein triggers (NPVTs) identified. The influence of these triggers on future recurrence is yet unknown.
BackgroundUse of pulmonary vein isolation (PVI) to treat atrialfibrillation continues to increase. Journal of the American Heart Association, Ahead of Print.
There are several approaches for provocation of non-pulmonary vein triggers (NPVTs) of atrialfibrillation (AF). However, it is unclear how these provocation efforts perform.
Targeting non-pulmonary vein triggers (NPVTs) after pulmonary vein isolation may reduce atrialfibrillation (AF) recurrence. Isoproterenol infusion and cardioversion of spontaneous or induced AF can provoke NPVTs but typically require vasopressor support and increased procedure time.
Bipolar voltage amplitude is capable of helping determine the ideal lesion size index (LSI) setting during radiofrequency (RF) ablation for atrialfibrillation (AF).
Patients with persistent atrialfibrillation (PeAF) may need additional ablation approaches on the basis of circumferential pulmonary vein isolation (PVI) to maintain long-term sinus rhythm. However, whether ablation of DZs in addition of PVI is effective in PeAF is unknown.
Following pulmonary vein isolation (PVI), about a third of patients have a very late recurrence (VLR) of atrialfibrillation (AF), defined as an AF recurrence after being free of AF for the first year following ablation. Additional data are needed to understand which patients remain at risk for VLR.
Pulmonary vein (PV) isolation is the cornerstone of radiofrequency (RF) ablation for atrialfibrillation (AF). PV reconnection is the most common cause of recurrent AF following an ablation procedure.
Background Pulmonary vein isolation with wide antral ablation leads to better clinical outcomes for the treatment of atrialfibrillation, but the isolation lesion is invisible in conventional cryoballoon ablation. The rate of 12-month freedom from clinical atrial arrhythmia recurrence was 85.1% min vs. 23.76 ± 8.36 min,
Rate vs Rhythm Control in AtrialFibrillation Rate vs rhythm control as a management strategy in atrialfibrillation has been a long standing topic for debate. EAST-AFNET 4 trial had 2789 patients with early atrialfibrillation and cardiovascular conditions [8]. years of follow up per patient.
While atrialfibrillation (AF) ablation has advanced to improve safety, success rates have been slower to improve. It has been shown that a lack of first-pass isolation (FPI) and the occurrence of acute pulmonary vein reconnection (PVR) predict AF recurrence.(1,2)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content