This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
So it must be atrialfibrillation. Then I always look to see if the initial deflection of the QRS has a lot of voltage change per change in time (seen in tachycardias that are initiated from above the ventricle because the propagate through fast conducting purkinje fiber. Pacemaker mediated tachycardia!
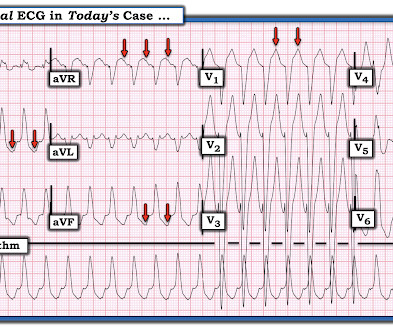
She also has a hx of paroxysmal atrialfibrillation and is on oral anticoagulant treatment. She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. The last echocardiography 12 months ago showed HFmrEF.
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation. What to do?
Here is the computer interpretation: ATRIALFIBRILLATION WITH RAPID VENTRICULAR RESPONSE WITH ABERRANT CONDUCTION OR VENTRICULAR PREMATURE COMPLEXES LEFT AXIS DEVIATION [QRS AXIS beyone -30] NONSPECIFIC ST and T-WAVE ABNORMALITY The over-reading physician confirmed this diagnosis, which is incorrect. It is not atrialfibrillation.
Ioannis Katsoularis, image courtesy of Klas Sjöberg milla1cf Thu, 12/14/2023 - 09:23 December 14, 2023 — Individuals infected with COVID-19 are also at an increased risk of suffering from heart rhythm disturbances, such as atrialfibrillation.
PMH: Known paroxysmal Atrial fib. He is usually is in sinus rhythm as far as he knows, but he cannot subjectively feel atrialfibrillation, so he is never completely certain when he is in sinus or atrial fib. Here is his ECG: Atrial Fib with a Ventricular Response of about 66. He immediately completely recovered.
BackgroundScreening for atrialfibrillation (AF) may reveal incidental arrhythmias of relevance. Among these were sinus node dysfunction in 14 patients (1.8%), AVB in 41 (5.2%), supraventricular tachycardia in 42 (5.3%), and ventricular tachycardia in 2 (0.3%). Journal of the American Heart Association, Ahead of Print.
Interpreting the waves and detecting abnormalities: Typically, the heart conducts electricity in a pathway starting in the sinoatrial node (SA), our heart’s “natural pacemaker”, located in the wall of the right atrium. Sinus tachycardia – sinus rhythm above 100 bpm is a sinus tachycardia.
This can initiate ventricular arrhythmias like polymorphic ventricular tachycardia (PMVT). Given the LV-RV offset of 40 msec, she would have received these two tightly coupled pacemaker spikes in an asynchronous mode, in this unfortunate instance during her T wave. Telemetry showed pacer spikes initiating PMVT.
It's a very "fun" ECG, with initial ectopic atrialtachycardia (negative P waves in inferior leads conducting 1:1 with the QRSs), followed by spontaneous resolution to sinus rhythm. Unfortunately the patient was erroneously diagnosed with "SVT / atrialfibrillation" and put on apixaban!!! What About the Tachycardia?
The aim of this study is to investigate the usefulness of an implantable loop recorder (ILR) for arrhythmia detection including atrialfibrillation (AF) in HFnon-rEF patients after discharge. Methods and analysis This is a multicentre single arm study to evaluate the usefulness of ILR for detecting arrhythmia.
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
AtrialFibrillationAtrialfibrillation causes irregular heartbeat, and the heart's normal blood supply is affected. Since atrialfibrillation can also be intermittent, such patients should continuously monitor their heart activity while performing daily activities with a portable ECG device.
Among 299 patients with CRT-pacemakers (BVP-111, LBBAP-188), VT/VF occurred in 8 patients in the BVP group vs. none in the LBBAP group (7.2% The occurrence of VT/VF was significantly lower with LBBAP compared with BVP (4.2% HR 0.46;95%CI 0.29-0.74;p<0.001). p<0.001). vs 0%;p<0.001). HR 0.46;95%CI 0.26-0.81;p=0.007).
ABSTRACT Background Catheter ablation (CA) for atrialfibrillation (AF) in the elderly poses a growing challenge. Methods Octogenarians with AF or consecutive atrialtachycardia undergoing index or re-ablation (pulmonary vein isolation [PVI] and ablation beyond PVI with different energy sources) in a single center, were analyzed.
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Negative predictors included dementia, pacemaker, coronary revascularization, and cerebrovascular disease. orthostatic vitals b.
How does a pacemaker accomplish RBBB morphology? Quick aside on device terminology (feel free to skip): A "single chamber" pacemaker is a device with only one lead. A "dual chamber" pacemaker is a device with an atrial lead and a ventricular lead. So the most likely rhythm in ECG 1 is ectopic atrialtachycardia.
2:34 PM, following right heart catheterization She then went into atrialfibrillation with complete heart block and junctional escape rhythm prompting placement of transvenous pacemaker. The catheter was out of the body and the arteriotomy had been closed, so there is no pressure waveform. Case discussion: This is a tragic case.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content