This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The patients were followed up for an average of 15 months by outpatient examination, telephone follow-up, or medical record inquiry of readmission patients. The patients were divided into standard-dose group (15–20 mg) and low-dose group (10–15 mg).
WHF characterized by outpatient intensification of oral loop diuretics is common yet its prognostic implications for ATTR-CM patients relative to other WHF events remains unclear. We assessed how WHF characterized by outpatient diuretic intensification (ODI) relates to mortality in this population. per 100 person-years; 95% CI 17.750.3)
What is the efficacy and safety of a single dose of 120 mg of flecainide acetate oral inhalation solution (FlecIH) administered in a monitored outpatient setting for the conversion of recent-onset atrialfibrillation (AF) to sinus rhythm (SR)?
Atrialfibrillation (AF) is the most common sustained cardiac rhythm disorder, affecting an estimated 43 million people globally. 1 Long-term AF management, including outpatient visits, hospitalisations and disabilities from stroke and heart failure (HF), adds substantial burden on healthcare resources and costs, accounting for 2.6%
Atrialfibrillation (AF) is the most common heart rhythm disorder in clinical practice. In this study, an electronic database of outpatients with AF, including patients with a history of COVID-19 infection was analyzed in order to assess the most significant risk factors for complications.
In previous randomized controlled trial, the alert system modestly enhanced the prescription of OAC among consecutive hospitalized patients with atrialfibrillation (AF).
Anticoagulation for stroke prevention is often recommended for patients with nonvalvular atrialfibrillation (AF), yet for variable reasons many eligible patients do not receive guideline-concordant anticoagulation. Prior quality improvement (QI) initiatives to improve anticoagulation in AF have had mixed results.
Objective The aim of this systematic review is to evaluate the various modalities available for extended ECG monitoring in the detection of atrialfibrillation (AF) following a cryptogenic stroke. Results 3924 studies were identified, of which 47 were included reporting on a pooled population of 6448 patients with cryptogenic stroke.
4 process measures were defined a priori: antithrombotic (AT) medication, high or medium potency statin, anticoagulation for atrialfibrillation (AF), and dual antiplatelet therapy (DAPT) 90 days or less after the consult completion. We collected administrative and chart review data for all neurology consults.
BackgroundThe economic burden of atrialfibrillation (AF) continues to increase. Thirtyday health service charges were calculated for ED visits, hospitalizations, and outpatient clinic appointments. Journal of the American Heart Association, Ahead of Print.
Background Atrialfibrillation (AF) represents a growing healthcare challenge, mainly driven by acute hospitalisations. Twenty-four of them avoided initial hospital admission as patients were directly enrolled to the virtual ward from outpatient settings.
Optimal NT-proBNP cut points for HFpEF rule out (optimizing sensitivity) and rule in (optimizing specificity) were derived and tested, stratified by obesity and atrialfibrillation.
Introduction:Continuous electrocardiographic monitoring using an implantable loop recorder (ILR) can facilitate the detection of asymptomatic atrialfibrillation episodes. The median time from implantation to the first detected atrialfibrillation was 115.7 The total positive detection of atrialfibrillation was 12 cases.
Background:A considerable portion of patients with embolic stroke of unknown source(ESUS)are later found to have occult atrialfibrillation (AF). Studies have shown that prolonged outpatient cardiac monitoring increases the chances of AF detection and impacts choice of antithrombotic therapy.
The average time to outpatient ICM placement was 57 days. Most inpatient ICM implants were performed by vascular and interventional neurology (n=181), and ICM use for cryptogenic stroke increased by 130%. The average time to inpatient ICM implant was 4.1 days, with 77% in 5 days and 95.5% within 10 days poststroke. AF detection rate of 36.5%
Abstract Introduction Despite advanced ablation strategies and major technological improvements, treatment of persistent atrialfibrillation (AF) remains challenging and the underlying pathophysiology is not fully understood. Patients were mainly suffering from long-standing persistent AF (mean AF duration 50.30 ± 54.28 months).
Choice of drugs for rate control is recommended based on left ventricular ejection fraction (LVEF), however, real-time assessment of LVEF remains limited, particularly in outpatient setting.
Atrialfibrillation (AF) is responsible for significant patient morbidity, and obesity is a major contributor to AF incidence and symptom burden. Individuals were screened following outpatient referral to Leeds Teaching Hospitals NHS Trust for symptomatic AF.
Background Cardiac arrhythmias have been observed among patients hospitalised with acute COVID-19 infection, and palpitations remain a common symptom among the much larger outpatient population of COVID-19 survivors in the convalescent stage of the disease. Median monitoring duration was 13.2 (IQR ventricular ectopic burden.
Continue reading to learn more about this procedure, its significance in treating atrialfibrillation, and what to expect during treatment. What is AtrialFibrillation? Before diving into electrical cardioversion, we should understand atrialfibrillation (AF). What Is Cardioversion?
ConclusionsWe identified substantial variation in the use of outpatient cardiac imaging related to physician and site factors. Generalized linear mixed‐effects models estimated the association of payment model (including the ability to bill to interpret imaging tests) and the use of cardiac imaging and quantified variation in cardiac imaging.
Patients could enter the study cohort upon receiving WATCHMAN or at an outpatient visit with an atrialfibrillation diagnosis, respectively. We used PS matching with a 1:3 ratio for patients in pLAAO and direct oral anticoagulant groups.
Methods We used the Swedish Registry of Cardiopulmonary Resuscitation, merged with the Inpatient Registry and Outpatient Registry to identify patients with OHCA from 2010 to 2020 and to collect all their comorbidities as well as discharge diagnoses (among those admitted to hospital). Previous AMI was prevalent in 14.8% of men and 10.9%
Adenosine is only unsafe in atrialfibrillation with WPW , which presents with a very rapid rate, polymorphic QRS, and some very short RR intervals] Bedside echo showed poor LV fct. But we just decided that we DON'T want a conversion to sinus until we can ascertain absence of thrombus in the atrial appendage!
Hopefully a repeat echocardiogram will be performed outpatient. Atrialfibrillation is also a predictor of worse outcomes in this case (Alborzi). Systolic function normal by visual assessment only, unable to visualize well for further characterization. 1900: RBBB and LAFB are almost fully resolved. No cardiac MRI was done.
Introduction:Catheter ablation (CA) is superior to medical therapy in the management of atrialfibrillation (AF). Stroke, Volume 56, Issue Suppl_1 , Page ATP283-ATP283, February 1, 2025. Current guidelines do not take into consideration the history of CA or its outcome when recommending chronic oral anticoagulation (OAC).
Simple eligibility criteria were based on data available in SwedeHF: heart failure as outpatient or at discharge from hospital, left ventricular ejection fraction 40%, N-terminal pro-B-type natriuretic peptide >300ng/L (in sinus rhythm) or>750ng/L (in atrialfibrillation), with pre-specified adjustment for elevated body mass index, and chronic (..)
vs. 54.7%, SD 0.6), and had a lower burden of atrialfibrillation (4.5% This finding sets the stage for future work leveraging both outpatient and pharmacy-based claims to further explore this finding. Patients with migraine were younger (40.2±15.2 standardized difference (SD) 0.38), more likely to be female (81.4%
Methods We collected information on HOCM patients followed-up at 25 Italian HCM outpatient clinics and with significant LVOTO (i.e. kg/m 2 p<0.0001) and a more frequent history of atrialfibrillation (21.5% Compared to the EXPLORER-HCM trial population, these RW HOCM patients were older (62.1±14.3 vs 9.8%, p=0.027).
Ensuring a follow-up neurology appointment within two weeks is vital to managing stroke risk factors like hypertension, diabetes, and atrialfibrillation. The clinic aims to support patients, manage stroke risk factors, and ensure a seamless transition to primary or outpatient neurology care.
Methods The ICM algorithm uses parameters derived from electrocardiogram (atrialfibrillation [AF], ventricular rate during AF, heart rate variability, and night heart rate), three-axis accelerometer (patient activity duration), and subcutaneous bioimpedance (fluid volume, respiration rate).
BACKGROUND:The mSToPS study (mHealth Screening to Prevent Strokes) reported screening older Americans at risk for atrialfibrillation (AF) and stroke using 2-week patch monitors was associated with increased rates of AF diagnosis and anticoagulant prescription within 1 year and improved clinical outcomes at 3 years relative to matched controls.
Unfortunately the patient was erroneously diagnosed with "SVT / atrialfibrillation" and put on apixaban!!! Hopefully his outpatient EP appointment will understand and correct that. See more posts on the atrial repolarization wave: K. [link] Electrolytes and TSH were normal. No use of drugs, stimulants, etc.
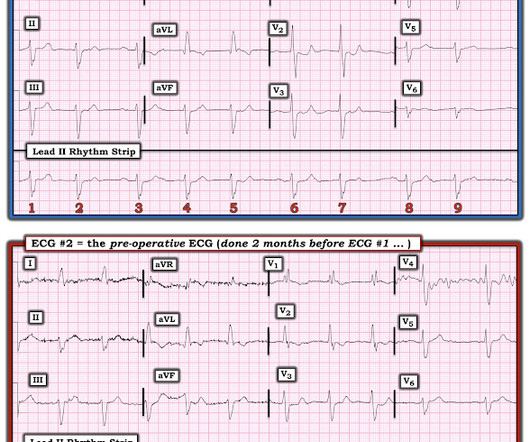
Here is the previous ECG from 2 months prior for pre-op for cataract surgery This appears to be atrialfibrillation with RBBB and LAFB. If the patient does not present with syncope, then outpatient management is probably OK, with referral to cardiology. This was interpreted as "AtrialFibrillation".
Laurent Fiorina, Cardiovascular Institute Paris-Sud (ICPS) and medical advisor for Philips, said: “Our main focus is developing new AI models to detect cardiovascular conditions or predict future cardiac events like atrialfibrillation, ventricular tachycardia, and now, severe bradyarrhythmia.”
The rhythm is atrialfibrillation. Initial ROSC was obtained, during which this ECG was obtained: What do you think? Meyers interpretation: This is a complicated interpretation made even more so by the fact that it is immediately post ROSC. The QRS complex is within normal limits.
Case sent by Magnus Nossen MD, edits by Meyers A previously healthy woman in her 60s presented to an outpatient clinic for palpitations. Today's CASE: To Review — The patient in today’s case is a previously healthy woman in her 60s who was seen in an outpatient clinic for “palpitations”.
We assessed the relationship of different ID definitions with cardiac structure and function, congestion, exercise capacity, and prognosis in HF outpatients. Conclusion In HF outpatients, TSAT <20% is more consistently associated with congestion by ultrasound and poorer functional capacity than other ID definitions, irrespective of LVEF.
Multivariable logistic regression analysis was used to determine the predictive value of the NNRS and KCCQ-OSS greater than the median values for NT-proBNP response with adjustment for age, sex, body mass index, comorbidities, baseline creatinine and NT-proBNP levels.
0.77];P<0.001), and lower atrialfibrillation risk (HR, 0.78 [95% CI, 0.65–0.93];P=0.006). Patients who underwent bariatric surgery were matched to controls in a 1:2 ratio (matched on exact age, sex, race, body mass index, HF encounter year, and HF hospitalization rate pre-surgery/matched period). 0.93];P=0.006).
We hypothesize the presence of comorbid cardiac disease has a synergistic effect on cognitive impairment in patients with asymptomatic CAS.Methods:Patients with 80% internal carotid artery stenosis with no history of stroke were recruited from inpatient and outpatient practices at a single, large, comprehensive stroke center.
Study Population includes all patients with an ischemic stroke inpatient admission in 2018 and were continuously enrolled with Medicare FFS for 1 year prior to and following their initial 2018 stroke admission. 1.378]), and heart failure (1.282 [95%CI, 1.25‐1.315]).ConclusionPatient
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content