This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background Heartfailure with preserved ejection fraction is a recognised outcome in patients with myocardial infarction, although heartfailure with reduced ejection fraction is more common. fold higher risk of heartfailure with preserved ejection fraction (95% CI 1.30 m/s had a 2.10-fold
Atrialfibrillation (AFib) is a common heart rhythm disorder characterized by an irregular and often rapid heartbeat. This condition can lead to various complications, including stroke and heartfailure, making it essential to understand its causes, symptoms, and AFib treatment options. What is AtrialFibrillation?
Background We evaluated the potential of circulating bone morphogenetic protein 10 (BMP10) as a biomarker for atrial stress and remodelling in patients with heartfailure (HF), in comparison to N-terminal pro-B-type natriuretic peptide (NT-proBNP). We also assessed the predictive value of BMP10 for adverse clinical outcomes.
Heartfailure (HF) is one of the significant complications in patients with myocardial infarction (MI), leading to increased risk for cardiovascular morbidity and mortality. 2 Therefore, early identification of HF in high-risk populations, particularly post-MI, is essential for improving outcomes. HFrEF is more commonly.
Background Atrialfibrillation (AF) and acute myocardial infarction (AMI) share risk factors and are bidirectionally associated. Several studies found higher risks of outcomes in individuals with both conditions. Whether the risks of outcomes differ according to temporal order of AF and AMI is unclear.
mtaschetta-millane Wed, 07/31/2024 - 06:00 July 31, 2024 — A novel study co-authored by a heartfailure cardiologist at University Hospitals Harrington Heart & Vascular Institute, demonstrates the effectiveness of a newly developed scoring system in identifying patients with HeartFailure with Preserved Ejection Fraction (HFpEF).
Atrialfibrillation is the most common cardiac arrhythmia worldwide with around 59 million people concerned in 2019. This irregular heartbeat is associated with increased risks of heartfailure, dementia and stroke. It gives early warnings on average 30 minutes before onset, with an accuracy of around 80%.
Outcomes of ablation with the FARAPULSE PFA System – a nonthermal treatment in which electric fields selectively ablate heart tissue – will be compared to outcomes following use of anti-arrhythmic drug (AAD) therapy, which is commonly prescribed for patients living with persistent AF. Circulation.
Initial causality was assessed by inverse variance weighting (IVW), followed by sensitivity analyses using MR-Egger regression, weighted median, and Multiple Effectiveness Residual Sums and Outliers (MR-PRESSO) method.
What is the prevalence of subclinical atrialfibrillation (AF) in patients with heartfailure and preserved ejection fraction (HFpEF), and how does it impact outcomes?
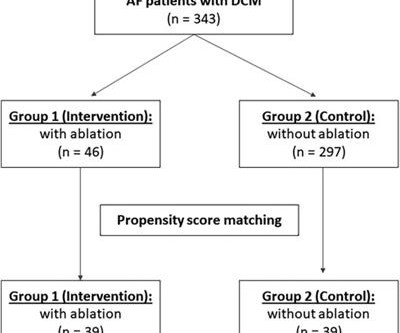
Introduction Catheter ablation is an effective and safe strategy for treating atrialfibrillation patients. Nevertheless, studies on the long-term outcomes of catheter ablation in patients with dilated cardiomyopathy are limited. Among the catheter ablation group, 58.7% ( n = 27) had persistent atrialfibrillation.
Introduction A high recurrence rate of atrialfibrillation was monitored after catheter ablation for persistent atrialfibrillation. The primary outcome will be sinus rhythm maintenance rate over 12 months, monitored by random electrocardiogram and 24-h Holter electrocardiogram.
Atrialfibrillation catheter ablation (AFCA) improved clinical outcomes compared with medical treatment alone, and early AFCA was associated with better outcomes than late AFCA, particularly decreased risk of heartfailure (HF) hospitalization and atrialfibrillation (AFib) recurrence.
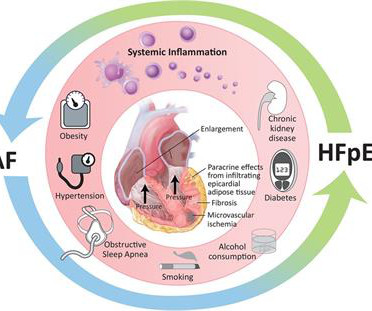
Heartfailure with preserved ejection fraction (HFpEF) and atrialfibrillation (AF) have emerged as major age-related epidemics within cardiology. Indeed, these two conditions are commonly found in the same individual, so much so that AF has been used in proposed diagnostic criteria for HFpEF.
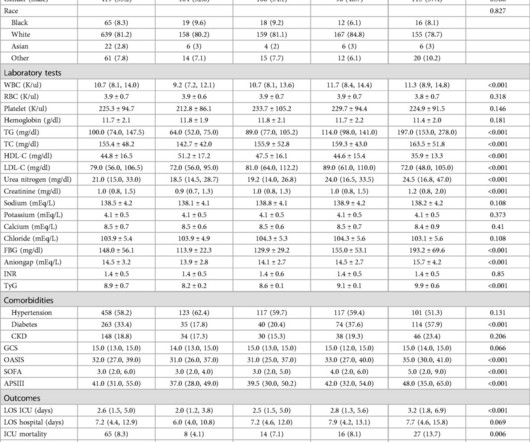
BackgroundThe role of the triglyceride-glucose (TyG) index in critically ill patients with congestive heartfailure (CHF) and atrialfibrillation (AF), requiring intensive care unit (ICU) admission, remains unclear. The primary outcome was hospital all-cause mortality.
The combined effect of left ventricular ejection fraction (LVEF) and atrialfibrillation (AF) on clinical outcomes in heartfailure (HF) remains complex.
Atrialfibrillation (AF) is a common arrhythmia in patients with heartfailure (HF). The coexistence of these conditions can further induce structural changes and result in worsened outcomes such as stroke, HF decompensation, poorly controlled AF, and mortality [1].
Discontinuation and reinitiation of mineralocorticoid receptor antagonists (MRA) in patients with heartfailure and reduced ejection fraction (HFrEF). BMI, body mass index; eGFR, estimated glomerular filtration rate; NYHA, New York Heart Association. 1.38), a diagnosis of atrialfibrillation (HR 1.24, 95% CI 1.10–1.39),
The term ‘epidemic’ is increasingly used to describe the rising global prevalence of atrialfibrillation (AF). Indeed, numerous studies are currently investigating the impact of such approaches on clinical outcomes and healthcare utilisation. Recent estimates suggest that AF accounts for between 0.9% 2 Before the.
The combined effect of Left Ventricular Ejection Fraction (LVEF) and the presence of AtrialFibrillation (AF) on clinical outcomes in heartfailure (HF) patients remains complex.
The impact of sodium-glucose cotransporter 2 inhibitors (SGLT2i) on atrialfibrillation (AF) recurrence outcomes and adverse cardiovascular outcomes in heartfailure (HF) patients after AF ablation is unknown.
Background Atrialfibrillation (AF) is common in individuals with heartfailure (HF). A statistically significant improvements in exercise capacity, heart disease QoL, anxiety and depression scores were observed within each group. Evidence supported the effect of exercise training in individuals with HF.
Clinical outcomes among patients with atrialfibrillation (AF) and heartfailure with preserved ejection fraction (HFpEF) treated with catheter ablation (CA) versus antiarrhythmic therapy (AAT) are not well-known.
Abstract A vast amount of now well-established clinical and epidemiological data indicates a close, interdependent, and symbiotic association between atrialfibrillation (AF) and heartfailure (HF). Both AF and HF, when co-exist in a patient, have serious treatment and prognostic implications.
Methods and results TRED-HF was a randomized trial investigating heartfailure therapy withdrawal in patients with recovered DCM over 6months. Clinical outcomes are reported in a non-randomized fashion from enrolment and from the end of the trial.
The authors claim that their score identifies heartfailure (HF) patients who benefit the most from atrialfibrillation (AF) ablation. More than identifying patients who benefit from the ablation, the score seems to identify patients who will have worse outcomes, irrespective of the treatment strategy.
Leukocyte telomere length (LTL) is a well-established biomarker linked to cardiovascular disease, with shorter LTL associated with increased severity of heartfailure (HF) outcomes. It is also well known that atrialfibrillation (AF) and HF are closely related and often coexist.
Studies have suggested that early atrialfibrillation (AF) ablation is associated with improved outcomes. However, it is unknown whether these patterns hold for persistent AF among patients with heartfailure with preserved ejection fraction (HFpEF). The majority of these studies evaluated paroxysmal AF cases.
Overview of the study population and effects observed after catheter ablation for atrialfibrillation. Conclusion Atrialfibrillation ablation in end-stage HF leads to a substantial decrease in AF burden, a regression from persistent to paroxysmal AF and notably improved LVEF. PVI, pulmonary vein isolation.
A number of studies have examined the impact of atrialfibrillation (AF) ablation on outcomes in heartfailure (HF) with reduced ejection (HFrEF) patients. In contrast, data from HF with preserved ejection fraction (HFpEF) patients is limited to small outcome studies and less robust meta-analyses.
Previous studies have demonstrated significant morbidity and mortality in patients with heartfailure (HF) with reduced ejection fraction (HFrEF), particularly with accompanying atrialfibrillation (AF).
Atrialfibrillation (AF) with comorbid heartfailure with preserved ejection fraction (HFpEF) presents a significant management challenge. While the association between AF and heartfailure with reduced ejection fraction is extensively studied, the correlation between AF and HFpEF remains less explored.
ABSTRACT Background Atrialfibrillation (AF) recurrence remains a significant challenge in heartfailure with reduced ejection fraction (HFrEF) patients undergoing cryoballoon ablation (CBA). This study assesses the impact of SGLT2i on AF recurrence and clinical outcomes in HFrEF patients undergoing CBA.
The prevalence of atrialfibrillation (AF) in patients with type 2 diabetes mellitus (T2DM) is reported to be higher than in the general population, ranging from 3.6% to 8.9 % [1].
Right ventricular (RV) function is an important predictor of outcomes in patients with heartfailure. The prevalence of RV dysfunction in patients with atrialfibrillation (AF) remains unclear.
Catheter ablation (CA) of atrialfibrillation (AF) has been proved to benefit patient with symptomatic AF and heartfailure. However, the data on neurological outcomes including cerebrovascular disease (CVA) and dementia remain a controversy.
Overtime, various studies have reported variable mortality outcomes in heartfailure with preserved ejection fraction (HFpEF) patients. It remains unclear to what extent atrialfibrillation (AF) creates increased mortality alone or in combination with either HFpEF or heartfailure with reduced ejection fraction (HFrEF).
The earlier indication of catheter ablation (CA) to atrialfibrillation (AF) had suggested the better outcome post-CA before advancement in left atrial remodeling. However, the optimal timing of CA in patients with a low burden of AF remains unknown.
Catheter ablation (CA) has become a cornerstone in the management of patients with comorbid atrialfibrillation (AF) and heartfailure with reduced ejection fraction (HFrEF). Multiple trials have demonstrated the efficacy of CA with respect to symptom improvement and quality of life in AF patients with HFrEF.
Catheter ablation(CA) is a class 1 indication in patients with atrialfibrillation (AF) and heartfailure with reduced ejection fraction (HFrEF). It is unclear whether complications differ in patients with HFrEF vs normal left ventricular ejection fraction(LVEF).
Atrialfibrillation often shortened to AFib is an irregular and often rapid heart rhythm that can lead to serious health complications. In some cases, AFib can also increase the risk of stroke, blood clots and heartfailure. The post How to Prevent an AtrialFibrillation Attack appeared first on AMS Cardiology.
So it must be atrialfibrillation. Answer : it is irregularly irregular and the initial part of the QRS is fast, so this is atrialfibrillation with Left Bundle Branch Block (LBBB). It stated that he had a non-ischemic cardiomyopathy, with EF of 15% and atrialfibrillation, and a normal angiogram 3 years prior.
The HFA–PEFF score comprising echocardiographic and laboratory data is designed to diagnose heartfailure with preserved ejection fraction and holds prognostic value in patients who underwent catheter ablation for atrialfibrillation (AF).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content