This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Jesse MacLaren guides us through 10 cases of patients who present with generalized weakness or acute neurologic symptoms and discusses how to look for ECG signs of dysrhythmias, electrolyte emergencies, acute coronary occlusion, and demand ischemia in patients with generalized weakness and in patients with neurologic symptoms, to consider predisposing (..)
Atrialfibrillation (AF) is the most common sustained cardiac dysrhythmia encountered in practice. It is currently estimated that AF affects approximately 2% of the general population; however, the true prevalence of AF is likely to be at least 3%–4% when asymptomatic AF is considered.
The differential of wide complex irregularly irregular includes: polymorphic VT, atrialfibrillation with WPW, atrialfibrillation with other aberrancy. Thus, the patients rhythm is atrialfibrillation with WPW. With that in mind, how would you proceed with treatment?
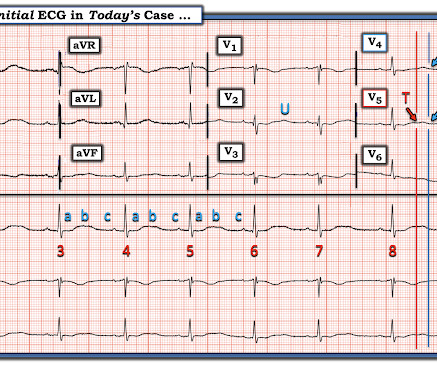
Especially when present in the setting of bradycardia and syncopal episodes, this is very worrisome for high risk of lethal dysrhythmias including polymorphic ventricular fibrillation (termed Torsades when in the setting of long QT). This ECG shows sinus bradycardia with massively long QT (or QU?) interval, at over 600 msec.
Here is the computer interpretation: ATRIALFIBRILLATION WITH RAPID VENTRICULAR RESPONSE WITH ABERRANT CONDUCTION OR VENTRICULAR PREMATURE COMPLEXES LEFT AXIS DEVIATION [QRS AXIS beyone -30] NONSPECIFIC ST and T-WAVE ABNORMALITY The over-reading physician confirmed this diagnosis, which is incorrect. It is not atrialfibrillation.
Regular means it can't be atrialfibrillation --Most regular wide complex tachcardia are VT, especially if the patient has poor LV function, as in this case. Relative contraindications to both include a known prolonged QT, especially if the dysrhythmia is believed to be caused by prolonged QT. What do you think?
In that sense, the term dysrhythmia is preferable because it does literally translate as a disturbance in normal rhythm which is exactly what it is meant to describe. Any unsolicited disturbance of the rate or rhythm can be termed a dysrhythmia and result in the heart beating less efficiently but only for the duration of the dysrhythmia.
Atrialfibrillation is also a predictor of worse outcomes in this case (Alborzi). See these publications for more information Overall, management for cardiac contusion is mostly supportive unless surgical complications develop, involving appropriate treatment of dysrhythmias and hemodynamic instability.
But adenosine only lasts for seconds, and if the dysrhythmia recurs, then the adenosine is gone. Prevent the initiation of the dysrhythmia -- this can be done with a beta blocker by prenenting PACS 2. This includes sinus tachycardia, atrialfibrillation or flutter, MAT, and others. Smith: should we give adenosine again?
There is atrialfibrillation. Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). Could the dysrhythmias have been prevented? This subsequent ECG was recorded after the K was up to 2.2
The rhythm is atrialfibrillation. Then there is loss of pulses with continued narrow complex on the monitor ("PEA arrest") Learning Points: Sudden witnessed Cardiac Arrest due to ACS is almost always due to dysrhythmia. Initial ROSC was obtained, during which this ECG was obtained: What do you think?
Inferior MI results in scar tissue which is a likely source of a re-entrant ventricular dysrhythmia. Knowing the rhythm is precisely regular rules out any possibility of atrialfibrillation — and facilitates calculation of heart rate. This would be the likely source of the VT.
Smith comment: In a large randomized trial of dopamine vs. norepinephrine (11) for shock which was published after the above-mentioned recommendations, dopamine had more adverse events (especially severe dysrhythmias, and especially atrialfibrillation).
Introduction:Patients with atherosclerotic carotid artery disease are at high risk of mortality in the long-term follow-up after carotid endarterectomy (CEA), partly due to dysrhythmia. Atrialfibrillation (AF) is a common cardiac dysrhythmia linked to stroke and cardiovascular events.
Here is one full text article on the topic from Clinical Cardiology 2008: Diagnostic Approach and Treatment Strategy in Tachycardia-induced Cardiomyopathy Atrial Tachycardia (AT): another SVT in the ED Rapid dysrhythmia from non-sinus focus above AV node.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content