This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Clinical introduction A woman in her 60s with non-obstructive coronaryarterydisease, aortic valve replacement and aortic arch repair, chronic diastolic heart failure and paroxysmal atrialfibrillation (AF) and flutter (AFL), presented with 3 days of sustained palpitations that felt similar to prior episodes of AF/AFL.
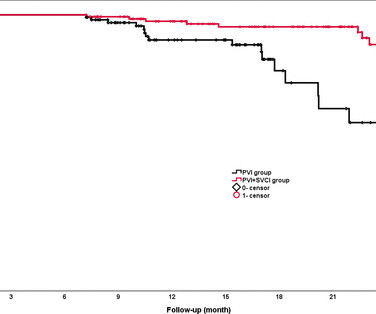
Background The value of empirical superior vena cava isolation (SVCI) following pulmonary vein isolation (PVI) to improve the efficacy of radiofrequency catheter ablation (RFCA) for paroxysmal atrialfibrillation (PAF) remains controversial.
Here is her ED ECG: Here is the ED physician's interpretation: IMPRESSION UNCERTAIN REGULAR RHYTHM, wide complex tachycardia, likely p-waves. LEFT BUNDLE BRANCH BLOCK [120+ ms QRS DURATION, 80+ ms Q/S IN V1/V2, 85+ ms R IN I/aVL/V5/V6] Comparison Summary: LBBB and tachycardia are new. This is clearly ventricular tachycardia.
Note: Due to the limited number of normally conducted beats — it is hard to be sure whether the underlying rhythm is sinus with baseline artefact or atrialfibrillation. A coronary angiogram was done that did not show significant coronaryarterydisease. There a two PVCs.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrialfibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. J Electrocardiol 2013;46:240-8 2.
The diagnostic coronary angiogram identified only minimal coronaryarterydisease, but there was a severely calcified, ‘immobile’ aortic valve. 3) Anemia, or poisons of hemoglobin such as methemoglobin or CO 4) Fixed coronary stenosis that limits flow. In the cath lab, the patient’s blood pressure remained low.
We identified the subset of variables most predictive of post‐HSCT cardiovascular events, defined as a composite of cardiovascular death, myocardial infarction, heart failure, stroke, atrialfibrillation or flutter, and sustained ventricular tachycardia.
An ECG or EKG monitor is used to detect diseases related to the heart. Here are the diseases that can be detected using an EKG monitor. AtrialFibrillationAtrialfibrillation causes irregular heartbeat, and the heart's normal blood supply is affected. It may be an intermittent or a permanent condition.
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronaryarterydisease with supply/demand mismatch). The rhythm now is atrialfibrillation. In the initial ECG (ECG# 1) aVR had ST elevation.
Written by Willy Frick with edits by Ken Grauer An older man with a history of non-ischemic HFrEF s/p CRT and mild coronaryarterydisease presented with chest pain. Additionally, the patient had no other apparent reason to have sinus tachycardia (such as volume depletion, bleeding, fever). ECG 1 What do you think?
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. However, there is also significant tachycardia , with heart rate of 116, and known hypoxia. The scan showed a bicuspid aortic valve with severe stenosis and coronaryarterydisease.
2:34 PM, following right heart catheterization She then went into atrialfibrillation with complete heart block and junctional escape rhythm prompting placement of transvenous pacemaker. Circumstances attending 100 sudden deaths from coronaryarterydisease with coroners necropsies. Circulation , 125 (3), 491496.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content