This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chestpain. He was eating lunch when he had sudden onset chest pressure, 9/10, radiating to his back, with sweating and numbness in both hands. was discovered.
An elderly dialysis patient presented with chestpain. Here is her ECG: Regular Wide Complex Tachycardia. Here is her ECG: Regular Wide Complex Tachycardia. Regular means it can't be atrialfibrillation --Most regular wide complex tachcardia are VT, especially if the patient has poor LV function, as in this case.
Written by Bobby Nicholson MD and Pendell Meyers A man in his 30s presented to the ED for evaluation of chestpain and palpitations. The ECGs show a wide complex, irregularly irregular tachycardia. Thus, the patients rhythm is atrialfibrillation with WPW. Thus, the patients rhythm is atrialfibrillation with WPW.
He had no chestpain or shortness of breath. But it is not disorganized enough to be polymorphic ventricular tachycardia. The rhythm is therefore atrialfibrillation with WPW until proven otherwise. Learning Points: Wide complex irregularly irregular tachycardias include PMVT, AF with WPW, and AF with aberrancy.
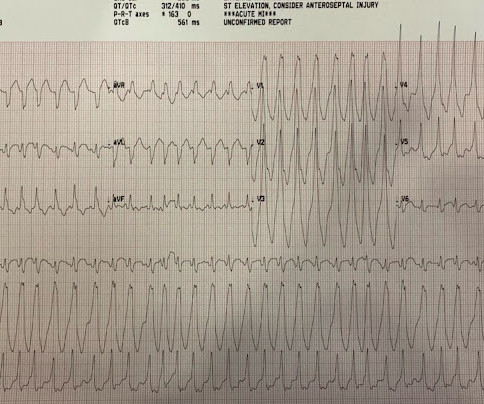
A prehospital 12-lead was recorded: There is a regular wide complex tachycardia. The computer diagnosed this as Ventricular Tachycardia. There is a wide complex regular tachycardia at a rate of 226. Toothache, incidental Wide Complex Tachycardia Could it be fascicular VT or Bundle Branch VT ( i.e., idiopathic VT )?
A 30-something presented with chestpain, palpitations, and SOB. The two ECGs above were texted to me with the text: "Young Guy came in in SVT but now in and out of irregular wide complex tachycardia. -- not sure if polymorphic VT vs. a fib with WPW." Definitely atrialfibrillation. Irregularly irregular 2.
She also has a hx of paroxysmal atrialfibrillation and is on oral anticoagulant treatment. She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. She presented to the emergency department after a couple of days of chest discomfort. Are you confident there is no ischemia?
This 60-something with h/o COPD and HFrEF (EF 25%) presented with SOB and chestpain. It is not atrialfibrillation. The rhythm is indeed irregularly irregular, so atrialfibrillation must be considered. Multifocal AtrialTachycardia 2. Here is the ECG: What do you think?
CT of chest showed the bullet path through his right lung but nowhere near his heart. There were times when it would be usurped by sinus tachycardia, then return to this rhythm. There is no atrial activity to suggest atrialfibrillation. But he did get an EKG: What is this? There is a wide complex. It is irregular.
In the evening, a middle-aged man complained of chestpain at the nursing home. His chestpain was vague. He mentioned "cancer" and "chest". He mentioned "cancer" and "chest". There is a narrow complex tachycardia at a rate of 130. The patient converted to atrialfibrillation.
BACKGROUND:Inflammation may promote atrialfibrillation (AF) recurrence after catheter ablation. Colchicine did not prevent atrial arrhythmia recurrence at 2 weeks (31% versus 32%; hazard ratio [HR], 0.98 [95% CI, 0.59–1.61];P=0.92) Circulation: Arrhythmia and Electrophysiology, Ahead of Print. 2.02];P=0.89). 1.99];P=0.55).CONCLUSIONS:Colchicine
Written by Willy Frick A 57 year old man with was admitted to the hospital with chestpain. The team immediately paged cardiology, concerned for polymorphic ventricular tachycardia. Since sinus conducted QRS complexes cannot co-exist together with ventricular tachycardia, this must all be artifact.
Chest trauma was suspected on initial exam. The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma? He was intubated for altered mental status.
His previous echo one month prior shows the same thing: “consistent with old infarct in LAD vascular territory, with EF 45%” "I think there is something else causing his tachycardia which is exaggerating his EKG findings and mimicking an acute myocardial infarction." Looks like atrialfibrillation. Cath lab was cancelled.
Here is her ED ECG: Here is the ED physician's interpretation: IMPRESSION UNCERTAIN REGULAR RHYTHM, wide complex tachycardia, likely p-waves. LEFT BUNDLE BRANCH BLOCK [120+ ms QRS DURATION, 80+ ms Q/S IN V1/V2, 85+ ms R IN I/aVL/V5/V6] Comparison Summary: LBBB and tachycardia are new. This is clearly ventricular tachycardia.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The history in today's case with sudden loss of consciousness followed by chestpain is very suggestive of ACS and type I ischemia as the cause of the ECG changes. The rhythm now is atrialfibrillation.
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Recently diagnosed with intermittent paroxysmal atrialfibrillation but no EKGs available to confirm. Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Sinus tachycardia does not go this fast.
If you experience any symptoms, such as chestpain, dizziness, unusual tiredness or fatigue, shortness of breath, or irregular heartbeat, your doctor would want you to go for an ECG test to find out the underlying cause. AtrialFibrillationAtrialfibrillation causes irregular heartbeat, and the heart's normal blood supply is affected.
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. The rhythm is atrialfibrillation. Chestpain, SOB, Precordial T-wave inversions, and positive troponin.
All of the patients presented with chestpain , and they are all in triage. Another frequent feature of hypothermia is atrialfibrillation (not seen in this case) Core temperature of this patient was 29,5 Celsius. Which, if any, of these patients has OMI, with myocardium at risk and need for emergent PCI?
ACS QID 75345 In 2017, the New England Journal of Medicine published the results of the Dual Antithrombotic Therapy with Dabigatran after PCI in AtrialFibrillation (RE-DUAL PCI) trial. His exam was notable for tachycardia, elevated jugular venous pressure, diffuse rales, and an early 2/6 systolic murmur loudest at the cardiac apex.
She reports that she is now unable to vagal out of her palpitations and is having shortness of breath and dull chestpain. We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. Now the patient is in sinus tachycardia. Sinus tachycardia, AFlutter and ATach do not do this.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrialfibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. A normal PR interval.
Answer : you must treat the patient's underlying condition causing sinus tachycardia, and repeat the ECG at the lower heart rate. Rate correction should not be used when RR interval has large variability, as in atrialfibrillation. Correlation of QT Interval Correction Methods During AtrialFibrillation and Sinus Rhythm.
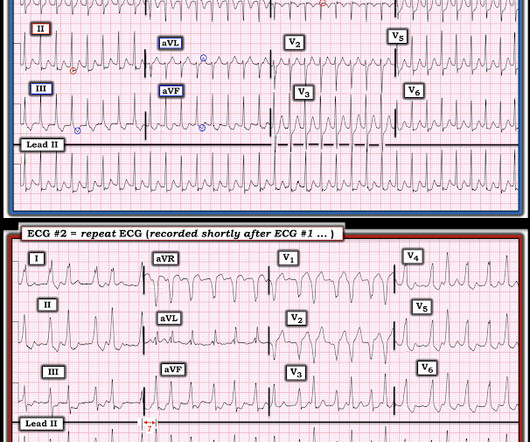
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia. MY Thoughts on the ECG in Figure-1: The rhythm in ECG #1 — is sinus tachycardia at ~125/minute.
A late middle-aged man presented with one hour of chestpain. There is atrialfibrillation. Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). Most recent echo showed EF of 60%.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. This was contributed by some folks at Wake Forest: Jason Stopyra, Shannon Mumma, Sean O'Rourke, and Brian Hiestand.
This middle-aged man with no cardiac history but with significant history of methamphetamin and alcohol use presented with chestpain and SOB, worsening over days, with orthopnea. Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. BP:143/99, Pulse 109, Temp 37.2 °C
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Most physicians will automatically be worried about these symptoms.
Written by Willy Frick with edits by Ken Grauer An older man with a history of non-ischemic HFrEF s/p CRT and mild coronary artery disease presented with chestpain. He said he had had three episodes of chestpain that day while urinating. So the most likely rhythm in ECG 1 is ectopic atrialtachycardia.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
2:34 PM, following right heart catheterization She then went into atrialfibrillation with complete heart block and junctional escape rhythm prompting placement of transvenous pacemaker. He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. Case discussion: This is a tragic case.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content