This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
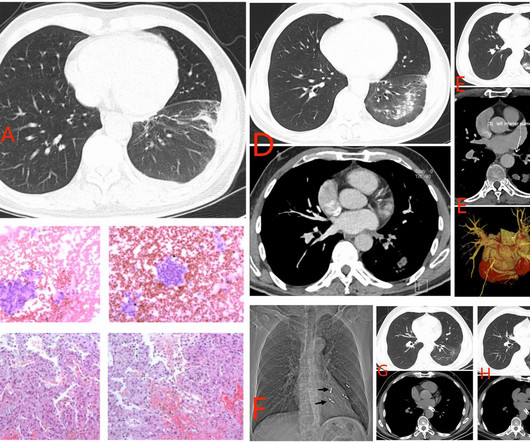
The increased use of radiofrequency ablation (RFA) for atrialfibrillation (AF) has led to a rise in cases of pulmonary vein stenosis or occlusion (PVS/O) as a complication. Clinical signs of PVS/O post-ablation can vary from no symptoms to common respiratory issues like coughing, hemoptysis, shortness of breath, and chestpain.
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chestpain. He was eating lunch when he had sudden onset chest pressure, 9/10, radiating to his back, with sweating and numbness in both hands. was discovered.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chestpain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrialfibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chestpain associated with nausea/vomiting 30 min PTA.
Whenever a patient does not have chestpain, the pre-test probability of OMI is diminished. Of course SOB, jaw pain, shoulder pain, etc can be a result of OMI, but the pretest probability is less and so you must scrutinize further. It is NOT only atrial paced, it is ventricular paced. The ECG: 1. was elevated.
He had no chestpain or shortness of breath. The rhythm is therefore atrialfibrillation with WPW until proven otherwise. Written by Pendell Meyers A teenager was playing basketball when he suddenly developed palpitations and lightheadedness. He presented soon afterward at the Emergency Department with ongoing symptoms.
A 50-something man presented in shock with severe chestpain. What is the atrial activity? Or is it atrialfibrillation with complete AV block and junctional escape? His prehospital ECG was diagnostic of inferior posterior OMI. The patient was in clinical shock with a lactate of 8.
A 30-something presented with chestpain, palpitations, and SOB. Definitely atrialfibrillation. Probably WPW but is very slow for atrial fib withWPW. So this looks like WPW with Atrialfibrillation. He has had similar symptoms for 4 years, but has never been evaluated. Irregularly irregular 2.
Written by Bobby Nicholson MD and Pendell Meyers A man in his 30s presented to the ED for evaluation of chestpain and palpitations. The differential of wide complex irregularly irregular includes: polymorphic VT, atrialfibrillation with WPW, atrialfibrillation with other aberrancy.
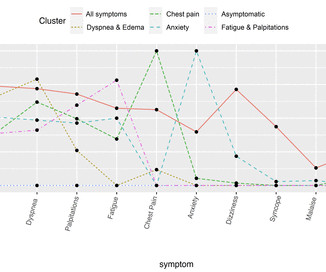
Objective This study aims to leverage natural language processing (NLP) and machine learning clustering analyses to (1) identify co-occurring symptoms of patients undergoing catheter ablation for atrialfibrillation (AF) and (2) describe clinical and sociodemographic correlates of symptom clusters.
There is no atrial activity to suggest atrialfibrillation. There are what could be interpreted as delta waves if, and only if, there were P-waves or other atrial activity preceding the QRS (pre-excitation can only happen when there is an impulse originating in the atria). There is a wide complex. It is irregular.
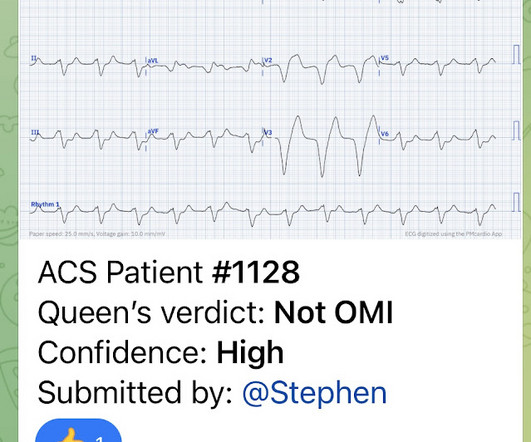
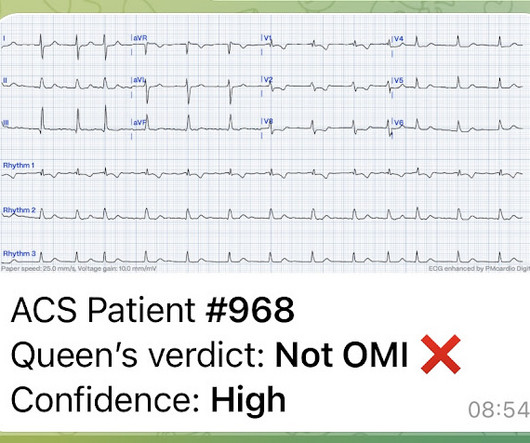
An 80-something woman who presented with chestpain and dyspnea. The rhythm appears to be atrialfibrillation. That said — QOH is already highly sophisticated and accurate in her assessment of ECGs from acute chestpain patients, in which the ECG is not complicated by uncommon OMI mimics. What do you think?
This 60-something with h/o COPD and HFrEF (EF 25%) presented with SOB and chestpain. It is not atrialfibrillation. The rhythm is indeed irregularly irregular, so atrialfibrillation must be considered. Multifocal Atrial Tachycardia 2. The patient in this case presented with dyspnea and chestpain.
Clinical introduction Vignette A woman in her 50s, with a history of atrialfibrillation, was admitted for a coronary angiography (CA) due to dyspnoea on exertion with a reduced ejection fraction of 40%. After 24 hours, the patient was readmitted to the hospital with chestpain and troponin elevation, without ECG changes.
BACKGROUND:Inflammation may promote atrialfibrillation (AF) recurrence after catheter ablation. Colchicine did not prevent atrial arrhythmia recurrence at 2 weeks (31% versus 32%; hazard ratio [HR], 0.98 [95% CI, 0.59–1.61];P=0.92) Circulation: Arrhythmia and Electrophysiology, Ahead of Print. 2.02];P=0.89). 1.99];P=0.55).CONCLUSIONS:Colchicine
An elderly dialysis patient presented with chestpain. Regular means it can't be atrialfibrillation --Most regular wide complex tachcardia are VT, especially if the patient has poor LV function, as in this case. She has poor LV function. Severely decreased LV function. Here is her ECG: Regular Wide Complex Tachycardia.
BackgroundAmiodarone is a class III antiarrhythmic drug that is commonly used in the clinic to treat ventricular arrhythmias and atrialfibrillation. Despite normal annual check-ups, she developed abnormal liver and thyroid function tests, and imaging revealed lung and liver changes suggestive of amiodarone toxicity.
Her Apple Watch suddenly told her that she is in atrialfibrillation. She did notice something slightly wrong subjectively, but had no palpitations, chestpain, or SOB, or any other symptom. Facilitating Transthoracic Cardioversion of AtrialFibrillation with Ibutilide Pretreatment. So it is safe.
Getty Images milla1cf Fri, 12/08/2023 - 08:17 December 8, 2023 — The American College of Cardiology (ACC) and the American Heart Association (AHA), along with several other leading medical associations, have issued a new guideline for preventing and optimally managing atrialfibrillation (AFib).
In the evening, a middle-aged man complained of chestpain at the nursing home. His chestpain was vague. He mentioned "cancer" and "chest". The patient converted to atrialfibrillation. Nurses found him with a BP of 50/30 and heart rate of 130 and called EMS. Fluids were started.
A 50 something male was seen in the emergency room due to typical chestpain. The pain had started the same day about two hours prior to medical contact. The medical care providers ascribed the patient's chestpain to new onset atrialfibrillation with rapid ventricular response after having viewed the ECG.
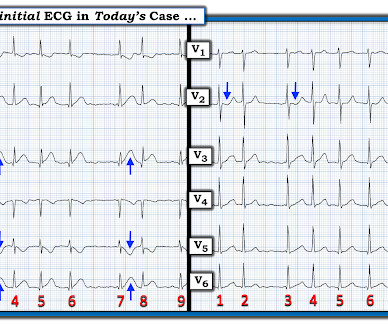
ECG from 2 days later: AtrialFibrillation now. My THOUGHTS on ECG #1: We are told that the patient in today’s case had an episode of severe chestpain 3 nights prior to admission. --Regional wall motion abnormality--mid to apical anterior hypokinesis. Inverted Reperfusion T-waves inferior Learning Points: 1.
milla1cf Thu, 01/18/2024 - 14:21 January 18, 2024 — Abbott announced the first global procedures have been conducted using the company's new Volt Pulsed Field Ablation (PFA) System to treat patients battling common abnormal heart rhythms such as atrialfibrillation (AFib).
Younger age (G1-G2-G3) was associated with a higher frequency of chestpain, pericardial rubs (p<0001), ECG changes (p=0.002) and were more commonly treated with colchicine (p<0.001), and non-steroidal anti-inflammatory drugs (p=0.006). Results A total of 471 patients (median age 56.3 (IQR IQR 33–73) years, 32.3%
Patient Mr. Paras Ram was having unstable angina (chestpain at rest) at his native place. He was in atrialfibrillation (irregular heart beat) too. The patient's atrialfibrillation also converted to good normal sinus rhythm after bypass surgery. All his coronary arteries were heavily calcified.
years]) admitted to the China ChestPain Center Database between 2016 and 2021. Hierarchical clustering of 15 medical conditions was performed to derive multimorbidity patterns. The primary outcome was a composite of inhospital adverse events.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
Abstract Introduction Left atrial appendage (LAA) closure (LAAC) is considered a viable alternative to anticoagulation therapy for stroke prevention in nonvalvular atrialfibrillation, we report a case with a less common shunt resulting from a device-related coronary artery-appendage fistula (CAAF) following LAAC.
24 will focus on the following three current guideline updates: American College of Cardiology (ACC)/American Heart Association (AHA) Guidelines 2023 AtrialFibrillation Guideline - Pharmacology II: Strokes vs. Bleeds, What Do the Guidelines Tell Us About Practical Management in A-fib? The Guidelines Sessions at ACC.24
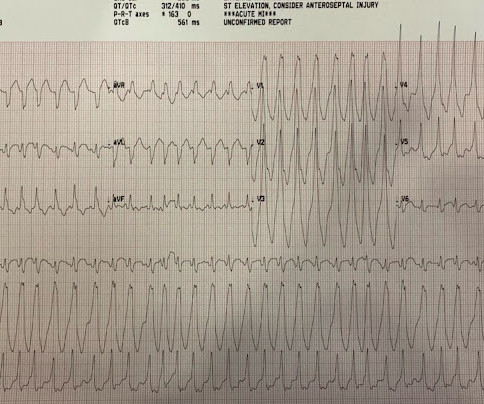
RVOT VT: A 40-something without past history presents with wide complex tachycardia and crushing chestpain Regular Wide Complex Tachycardia. It is dangerous in WPW with atrialfibrillation. In AtrialFibrillation, the tachycardia will always be irregularly irregular. There is no inferior axis.
On this month's EM Quick Hits podcast David Carr on differential diagnosis of normal unenhanced CT renal colic, Leeor Sommer on recognition and management of perichondritis and auricular abscess, Suzanne Schuh on IV magnesium sulphate for pediatric asthma, Jess McLaren on Occlusion MI ECG interpretation requiring cath lab activation and Justin Morgenstern (..)
Diagnosis : Atrial flutter with 1:1 conduction, with fast AV conduction made possible by sympathetic drive of exercise On arrival, we obtained another 12-lead: Unremarkable Further history: One month history of shortness of breath on exertion, denies palpitations, chestpain, orthopnea, leg swelling.
These include breathlessness, chestpain, dizziness or even blackouts. Tags: arrhythmia; dysrhythmia; heart palpitations; anxiety; heart disease; atrialfibrillation; sanjay gupta; yorkcardiology The post WHAT EXACTLY IS AN ARRHYTHMIA? The diagnosis of a dysrhythmia is made by recording an ECG during the dysrhythmia.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrialfibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting.
She also has a hx of paroxysmal atrialfibrillation and is on oral anticoagulant treatment. She presented to the emergency department after a couple of days of chest discomfort. The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. The last echocardiography 12 months ago showed HFmrEF.
He was brought to the critical care area where these rhythms were seen on the monitor: Wide complex tachycardia with no apparent P-waves, and very irregular Consistent with atrialfibrillation with aberrancy A Regular wide complex tachycardia. Looks like atrialfibrillation. LV Aneurysm? Would you give Thrombolytics?
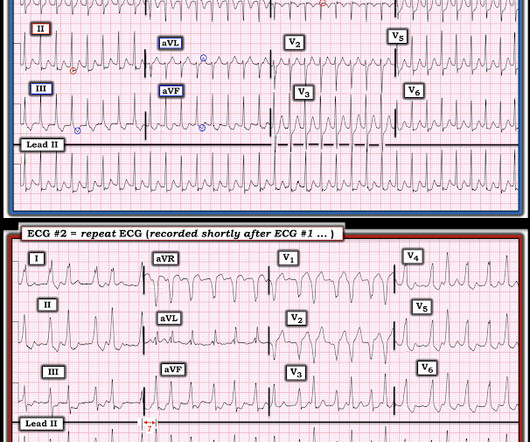
She reports that she is now unable to vagal out of her palpitations and is having shortness of breath and dull chestpain. The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrial flutter with regular conduction. This includes sinus tachycardia, atrialfibrillation or flutter, MAT, and others.
While specific criteria to assess hemodynamic stability include the presence ( or absence ) of arrhythmia-related hypotension, chestpain, shortness of breath, and/or mental status changes — an overall “Gestalt” assessment from “being there” (ie, at the patient’s bedside ) needs to be consciously made.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. This was contributed by some folks at Wake Forest: Jason Stopyra, Shannon Mumma, Sean O'Rourke, and Brian Hiestand.
28, 2025 At theAmerican College of Cardiology (ACC) 2025 meeting,GE HealthCare will introduce RevolutionVibe, i a new computed tomography (CT) system with Unlimited One-Beat Cardiac imaging to deliver consistent, high-quality images for patients, even in challenging cases like atrialfibrillation and heavily calcified coronaries.
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? Conduction and refractoriness alternans may be seen with WPW-related as well as AV Nodal-dependent reentr y tachycardias — atrialfibrillation — acute pulmonary embolus — myocardial contusion — and severe LV dysfunction.
milla1cf Wed, 12/13/2023 - 10:24 December 13, 2023 — A new artificial intelligence (AI) model designed by Scripps Research scientists could help clinicians better screen patients for atrialfibrillation (or AFib)—an irregular, fast heartbeat that is associated with stroke and heart failure.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The history in today's case with sudden loss of consciousness followed by chestpain is very suggestive of ACS and type I ischemia as the cause of the ECG changes. The rhythm now is atrialfibrillation.
Written by Willy Frick A 57 year old man with was admitted to the hospital with chestpain. Such as atrialfibrillation or sinus rhythm with extrasystoles. Answer shown below: This can be even more challenging with atrialfibrillation where the only thing you can rely on is careful morphologic inspection.
All of the patients presented with chestpain , and they are all in triage. Another frequent feature of hypothermia is atrialfibrillation (not seen in this case) Core temperature of this patient was 29,5 Celsius. Which, if any, of these patients has OMI, with myocardium at risk and need for emergent PCI?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content