This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
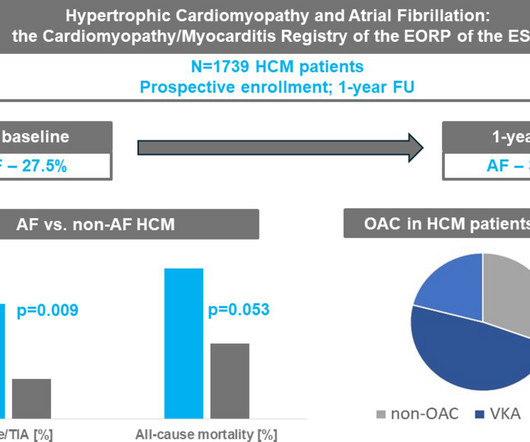
Background Hypertrophic cardiomyopathy (HCM) is commonly associated with atrialfibrillation (AF), but its impact on outcomes in real-world practice is uncertain. years) were enrolled in the EURObservational Research Programme (EORP) Cardiomyopathy/Myocarditis Registry. Methods Overall, 1739 adult patients with HCM (40.9%
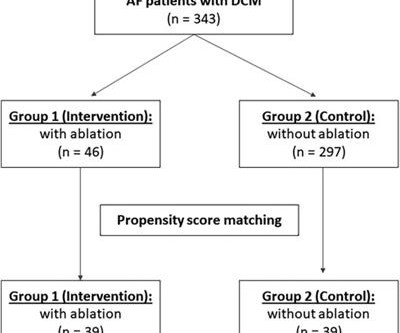
Introduction Catheter ablation is an effective and safe strategy for treating atrialfibrillation patients. Nevertheless, studies on the long-term outcomes of catheter ablation in patients with dilated cardiomyopathy are limited. Among the catheter ablation group, 58.7% ( n = 27) had persistent atrialfibrillation.
When atrialfibrillation (AF) begins, it can start with a single focus, degenerating to multiple wavelets, and it spreads throughout the entire surface area of both atria. A fibrillatory wave that occurs at a rate of more than 600 beats per minute can cause fatigue in the long run, leading to atrial dilation.
Keywords with strong recent citation bursts included tissue, cardiomyopathy, and closed chest ablation.ConclusionPFA is becoming established as a viable alternative for AF ablation, showing promising safety and efficacy. Prolific authors were identified, underscoring significant international collaborations.
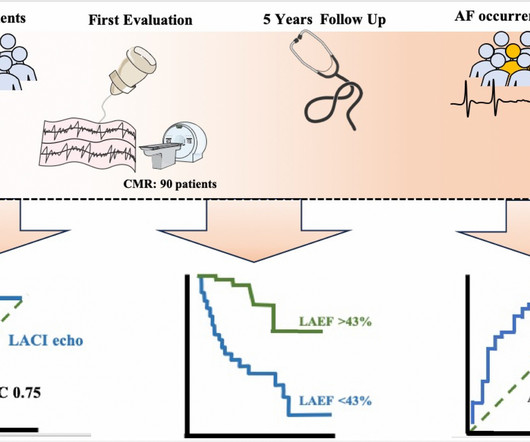
Several predictors of atrialfibrillation (AF) onset in patients with hypertrophic cardiomyopathy (HCM) have been proposed, however, all of them showed limited accuracy. This study aims to assess the role of n.
So it must be atrialfibrillation. Answer : it is irregularly irregular and the initial part of the QRS is fast, so this is atrialfibrillation with Left Bundle Branch Block (LBBB). Patient has an ICD, which is primarily placed in patients with cardiomyopathy. What do you think? mm; the S-wave is 18 mm.
We thank Hundal and colleagues for their letter1 regarding our analysis of the incidence of new-onset and progressive atrialfibrillation (AF) in mavacamtent-treated patients with obstructive hypertrophic cardiomyopathy (oHCM)2.
male with pertinent past medical history including Atrialfibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Of course, this is NOT atrial fib, but rather PSVT, and so adenosine should work.
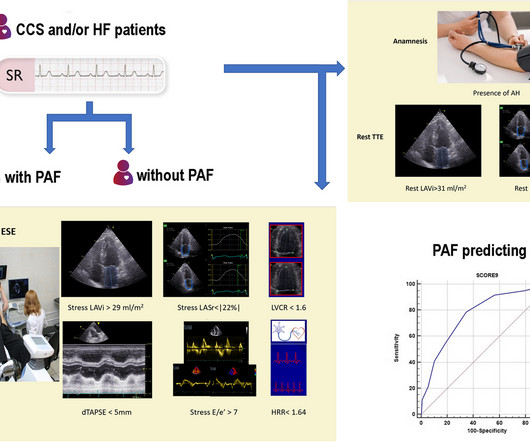
Atrialcardiomyopathy is closely associated with atrialfibrillation (AF), and some patients exhibit no dysfunction at rest but demonstrate evident changes in left atrial (LA) function and LA volume during exe.
Catheter ablation of atrialfibrillation in infiltrative cardiomyopathies ABSTRACT Atrial and ventricular arrhythmias are common in patients with Infiltrative heart diseases. Catheter ablation is a safe and effective modality for the treatment of AF in infiltrative cardiomyopathy.
Percutaneous left atrial appendage closure (LAAC) is an effective alternative strategy for stroke prevention in atrialfibrillation (AF) patients at high risk for bleeding with anticoagulation (AC). Efficacy of this strategy in hypertrophic cardiomyopathy (HCM) remains uncertain.
Atrialfibrillation(AF) is associated with increased risk of embolic stroke and heart failure hospitalizations in patients with hypertrophic cardiomyopathy(HCM).
Oral diuretic intensification was significantly prognostic of mortality amongst patients with transthyretin cardiomyopathy and occurred more often than HF hospitalization. Patients experiencing ODI had higher rates of subsequent mortality (17.7 per 100 person-years; 95% confidence interval [CI] 13.323.7) per 100 person-years; 95% CI 17.750.3)
American College of Cardiology (ACC) and American Heart Association (AHA) Issue New Hypertrophic Cardiomyopathy (HCM) Management Guidelines 2. Late-breaking Clinical Trial Results from FARADISE, admIRE Study and Advent Trial at Heart Rhythm 2024 Highlight Pulsed Field Ablation Developments for AtrialFibrillation Treatment 8.
Development of a machine learning model to predict new-onset atrialfibrillation in patients with hypertrophic cardiomyopathy. Aims Atrialfibrillation (AF) is the most common sustained arrhythmia among patients with hypertrophic cardiomyopathy (HCM), leading to increased symptom burden and risk of thromboembolism.
study on the frequency of new-onset and recurrent atrialfibrillation (AF) events in patients with obstructive hypertrophic cardiomyopathy (oHCM) on mavacamten.1 We read with interest Castrichini et al.s
BackgroundClinical and genetic predispositions are significant in predicting atrialfibrillation (AF); however, their role in patients with hypertrophic cardiomyopathy (HCM) remains unclear. Journal of the American Heart Association, Ahead of Print.
In this weeks View, Dr. Eagle looks at arrhythmia recurrence and rhythm control after catheter ablation for atrialfibrillation. He then discusses long-term outcomes in transthyretin amyloid cardiomyopathy in patients treated with tafamidis.
Atrialfibrillation (AF) is common in patients with hypertrophic cardiomyopathy (HCM) and can be challenging to manage. Atrioventricular nodal (AVN) ablation may be an effective management strategy for AF in these patients.
In patients with hypertrophic cardiomyopathy (HCM), atrialfibrillation (AF) poses significant clinical challenges because of its adverse impact on hemodynamics. AF, especially when accompanied by rapid ventricular responses, compromises atrial contraction and in turn increases diastolic filling of the left ventricle.
Mavacamten is a cardiac myosin inhibitor that has been shown to reduce left ventricular outflow tract obstruction in obstructive hypertrophic cardiomyopathy (oHCM).1 1 In late-stage clinical trials, atrialfibrillation (AF) represented an adverse event in 2-4 % of the patients randomized to mavacamten.1,2
Wild-type transthyretin amyloid cardiomyopathy (ATTRwt-CM) is often accompanied by atrialfibrillation (AF), atrial flutter (AFL), and atrial tachycardia (AT), which are difficult to control because beta-blockers and antiarrhythmic drugs can worsen heart failure (HF).
Mechanisms and potential targets to manage atrialfibrillation related to diabetes mellitus are represented. ABSTRACT In spite of significant progress made in the management in recent decades, atrialfibrillation (AF) continues to cause increased mortality and significant morbidities, including heart failure and stroke.
Long-term follow-up (FU) of the TRED-HF trial: persistent high-risk of relapse following therapy withdrawal in recovered dilated cardiomyopathy (DCM), likely contributed to by low-dose therapy and exposure to external triggers. LVEF, left ventricular ejection fraction. This follow-up investigates the longer-term effects of therapy withdrawal.
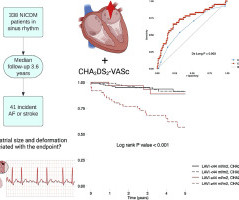
Abstract Introduction In hypertrophic cardiomyopathy (HCM), atrialfibrillation (AF) has historically been regarded to have a deleterious impact on clinical course, strongly associated with progressive heart failure (HF) symptoms. Results Among the 218 patients, 50 (23%) had a history of AF and comprise the primary study cohort.
ABSTRACT Background Atrialfibrillation and atrial flutter are relatively rare in young people and the incidence of thromboembolic complications is unknown. Structural heart disease (SHD) was present in 120 patients (57%) and 20 patients (10%) had a primary cardiomyopathy.
Atrialfibrillation (AF) has been known as a main cause of embolic stroke. Atrial mechanical remodeling presenting cardiomyopathy could lead to not only occur AF but also increase risk of thromboembolism.
Overview of the study population and effects observed after catheter ablation for atrialfibrillation. Electroanatomic mapping showed the extent of left atrial low voltage (cardiomyopathy) >10% in 31 (31.9%) patients. PVI, pulmonary vein isolation.
Atrialfibrillation (AF), a common cardiac arrhythmia, often results in significant atrial remodeling, including atrialcardiomyopathy and dilatation. Notably, aFMR is linked to a higher recurrence rate of AF after catheter ablation.
BackgroundCardiac myosin inhibitors were recently developed to address the underlying pathophysiology of hypertrophic cardiomyopathy and to improve symptoms and quality of life. versus 0.5%, respectively, in oHCM) due to left ventricular ejection fraction reduction, atrialfibrillation (11.5
ABSTRACT There is a parallel epidemic of atrialfibrillation (AF) and hypertension (HTN) occurring globally. The pathophysiological alterations and structural changes that occur in the atria, including architectural subcellular abnormalities fibrosis, are considered to cause atrialcardiomyopathy (atriopathy) predisposing to AF.
What is the impact of atrialfibrillation (AF) catheter ablation in patients with hypertrophic cardiomyopathy (HCM) on reduction in AF burden and symptoms?
A person’s LAA may create issues including atrialfibrillation and stroke. We have the extensive expertise to offer isolated minimally invasive left atrial appendage occlusion through left-sided video assisted surgery,” said Dr. Rushing, Director of the Surgical AtrialFibrillation program at UH Harrington Heart & Vascular Institute.
Publication date: Available online 26 September 2024 Source: The American Journal of Cardiology Author(s): Eduard Ródenas-Alesina, Jordi Lozano-Torres, Pablo Eduardo Tobías-Castillo, Clara Badia-Molins, Maria Calvo-Barceló, Rosa Vila-Olives, Guillem Casas-Masnou, Aleix Olivella San Emeterio, Toni Soriano-Colomé, Rubén Fernández-Galera, Ana B Méndez-Fernández, (..)
Atrialfibrillation (AF) in patients with hypertrophic obstructive cardiomyopathy (HOCM) may be caused by a primary atrial myopathy. Whether HOCM-related atrial myopathy affects mainly electrophysiological properties of the left atrium (LA) or also the right atrium (RA) has never been investigated.
Although atrialfibrillation/atrial flutter (AFib/AFL) are common manifestations of transthyretin amyloid cardiomyopathy (ATTR-CM), a post hoc analysis of the ATTR-ACT study, published April 30 in JACC: CardioOncology, found they do not predict all-cause mortality.
The EHRA/HRS/APHRS/SOLAECE Expert Consensus on AtrialCardiomyopathies published in 2017 defined atrialcardiomyopathy as “any complex of structural, architectural, contractile, or electrophysiological changes affecting the atria.”1
Atrialcardiomyopathy is known as an underlying pathophysiological factor in the majority of AF patients. Left atrial low-voltage areas (LVAs) are reported to coincide with fibrosis, and to likely represent atrialcardiomyopathy.
Atrialcardiomyopathy is a condition that causes electrical and contractile dysfunction of the atria, often along with structural and functional changes. Atrial enlargement and atrialfibrillation are common complications of ASCM and are often the predominant clinical features.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content