This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
While on telemetry monitoring he suffered cardiacarrest and was resuscitated. What ECG finding may have contributed to (or precipitated) the cardiacarrest? Note: The patient while on telemetry had alternating atrialfibrillation, sinus rhythm with 1st degree AV block and also periods of Wenckebach conduction.
So it must be atrialfibrillation. Answer : it is irregularly irregular and the initial part of the QRS is fast, so this is atrialfibrillation with Left Bundle Branch Block (LBBB). What do you think? Rhythm : Residents asked me why it is not VT. mm; the S-wave is 18 mm. So we should activate the cath lab, right?
Here was his initial ED ECG: There is atrialfibrillation with a rapid ventricular response. ST depression is common BOTH after resuscitation from cardiacarrest and during atrial fib with RVR. He had not complained of any premonitory symptoms (which is very common). He had a history of CAD with CABG.
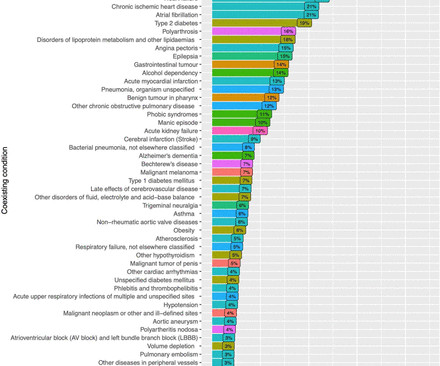
Background Out-of-hospital cardiacarrest (OHCA) has a dismal prognosis with overall survival around 10%. Previously, 80% of sudden cardiacarrest have been attributed to coronary artery disease. We studied comorbidities and discharge diagnoses in OHCA in all of Sweden. Previous AMI was prevalent in 14.8% of the men.
Rate vs Rhythm Control in AtrialFibrillation Rate vs rhythm control as a management strategy in atrialfibrillation has been a long standing topic for debate. EAST-AFNET 4 trial had 2789 patients with early atrialfibrillation and cardiovascular conditions [8]. years of follow up per patient. N Engl J Med.
Patient had an unwitnessed cardiacarrest without bystander CPR performed. Initial vitals show hypertension (175/85), AtrialFibrillation with RVR as seen in Figure 1 , hypercapnia (99mmHg), and SPO2 of 100%. After 5 minutes post-ROSC, the atrialfibrillation converted to a sinus rhythm.
The patient had a combined respiratory and metabolic acidosis (as we commonly find in those with prolonged arrest), and a K of 4.1, The rhythm is nearly regular, but there are no P-waves (it is too regular to be atrialfibrillation). at the time of the ECG. Mg was 1.6. However, the QRS is barely wide, if at all.
Written by Pendell Meyers First try to interpret this ECG with no clinical context: The ECG shows an irregularly irregular rhythm, therefore almost certainly atrialfibrillation. After an initially narrow QRS, there is a very large abnormal extra wave at the end of the QRS complex. There is also large T wave inversion and long QT.
The rhythm is atrialfibrillation. He had multiple cardiacarrests with ROSC regained each time. Then there is loss of pulses with continued narrow complex on the monitor ("PEA arrest") Learning Points: Sudden witnessed CardiacArrest due to ACS is almost always due to dysrhythmia.
Whenever it is this fast, you need to be very careful to ascertain whether it is irregular ( as in atrialfibrillation with rapid ventricular respsonse ) or regular ( as in VT ). This is not because it is polymorphic VT; it is because it is WPW with atrialfibrillation. Atrialfibrillation/flutter in pre-excitation.
Arrhythmias: Genetic mutations can also predispose individuals to irregular heart rhythms, such as atrialfibrillation or long QT syndrome, which may increase the risk of stroke or sudden cardiacarrest. Mutations in specific genes often cause hypertrophic cardiomyopathy and dilated cardiomyopathy.
Nearly two decades ago, an alarm was sounded about potential cardiac risks of stimulant medication (SM). The risk of cardiacarrest in WPW is due to rapid conduction of atrialfibrillation via the accessory pathway to the ventricles. The use of SM in Wolff-Parkinson-White (WPW) has not been well studied.
6 , the program will include, among networking and roundtables, the following: HRX Pitch Competition #1 CardiacArrest, the Next Digital Health Frontier: Mina K. Kathryn Zavala | Stephen Flaim | Giovanni Leo | Daniel Gottlieb | David Kim | David Roman During day two of HRX 2024, Friday, Sept.
AtrialFibrillationAtrialfibrillation causes irregular heartbeat, and the heart's normal blood supply is affected. Since atrialfibrillation can also be intermittent, such patients should continuously monitor their heart activity while performing daily activities with a portable ECG device.
Smith’s ECG Blog: SQTS is an inherited cardiac channelopathy determined by the presence of symptoms ( syncope, cardiacarrest ) — positive family history — and the ECG finding of an abnormally short QTc interval. SQTS is a relatively new diagnosis that has only been recognized as a distinct clinical entity since 2000.
The rhythm now is atrialfibrillation. This patient is actively dying from a left main coronary artery OMI and cardiacarrest from VT/VF or PEA is imminent! Complete LMCA occlusion is associated with clinical shock and/or cardiacarrest. A repeat ECG was recorded about 15 minutes after the initial ECG.
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. Cardiac Motion Alternans — is the result of cardiac movement rather than electrical alternation.
Logistic regression was used to analyze the relationship between the treatment groups and hospital readmission within 90 days.Results:Only 517 AA met inclusion criteria and did not meet exclusion criteria, which included a history of valvular heart disease, hypertrophic or restrictive cardiomyopathy, active myocarditis, history of cardiacarrest, and (..)
There is atrialfibrillation. Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). If cardiacarrest from hypokalemia is imminent (i.e., mEq/L: The STE is resolved. mEq/L, from 1.9
Osborn waves have been reported with hypercalcemia, brain injury, subarachnoid hemorrhage, Brugada syndrome, cardiacarrest from VFib — and — severe, acute ischemia resulting in acute MI ( See My Comment in the November 22, 2019 post on Dr. Smith’s Blog ). Rituparna et al — as well as Chauhan and Brahma ( Int.
Still more are factors are age < 18 years, sudden cardiac death in first degree relative, SCN5A mutations, atrialfibrillation, PR interval > 200 ms, QRS duration > 120 ms, presence of late potentials and aVR sign, manifested as R wave ≥ 0.3 Atrialfibrillation and Brugada syndrome. mV or R/q ≥ 0.75.
Another frequent feature of hypothermia is atrialfibrillation (not seen in this case) Core temperature of this patient was 29,5 Celsius. Smith: This bizarre ECG looks like a post cardiacarrest ECG with probable acidosis or hyperkalemia in addition to OMI. Troponins were negative in serial blood tests. Potassium 4,6.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrialfibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting.
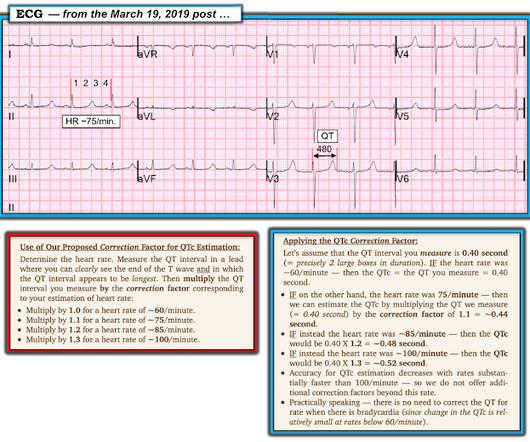
Rate correction should not be used when RR interval has large variability, as in atrialfibrillation. AtrialFibrillation: These authors compared Bazett, Fridericia, and Framingham QT measurements on 54 patients with atrialfibrillation. Dangerously prolonged QT is 480, especially greater than 500 ms.
Conduction and refractoriness alternans may be seen with WPW-related as well as AV Nodal-dependent reentr y tachycardias — atrialfibrillation — acute pulmonary embolus — myocardial contusion — and severe LV dysfunction. Cardiac Motion Alternans — is the result of cardiac movement rather than electrical alternation.
Background:Catheter ablation (CA) is increasingly used for treatment of atrialfibrillation (AF). Cox proportional hazards models were used to estimate hazard ratios (HR) for the composite and individual endpoints from CABANA trial (death, stroke, major bleeding or cardiacarrest) and CASTLE-AF trial (death or heart failure).
Smith’s ECG Blog: SQTS is an inherited cardiac channelopathy determined by the presence of symptoms ( syncope, cardiacarrest ) — positive family history — and the ECG finding of an abnormally short QTc interval. SQTS is a relatively new diagnosis that has only been recognized as a distinct clinical entity since 2000.
The final letter in the SLOWED mnemonic is " D " for "Dead" ( resulting from VT/VF or asystolic cardiacarrest ). In a sense — frequent ventricular ectopy is already included in this "D" ( which frees use of the "E" to prompt recall of ST elevation that may be seen with hypothermia, and which is not the result of acute OMI ).
Typical symptoms associated with HCM include atrialfibrillation (AF), syncope, ventricular fibrillation, and cardiacarrest. Phenotypically, the patient initially presented with syncopal episodes, atrioventricular (AV) block, and atrialfibrillation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content