This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
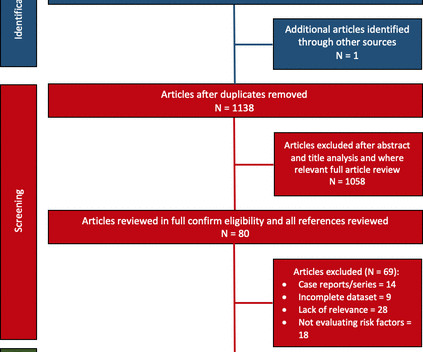
Bradyarrhythmia and atrialfibrillation (AF) incidence are reported in up to 16% and 13%, respectively. Objective We conducted a systematic review evaluating AF burden and bradycardia requiring permanent pacemaker (PPM) implantation and report any predictive risk factors identified.
Initial vitals show hypertension (175/85), AtrialFibrillation with RVR as seen in Figure 1 , hypercapnia (99mmHg), and SPO2 of 100%. Figure 1 : Initial ECG shows AtrialFibrillation with LBBB morphology and mild discordant STE not consistent with OMI. Atropine and further doses of epinephrine were not administered.
PMH: Known paroxysmal Atrial fib. He is usually is in sinus rhythm as far as he knows, but he cannot subjectively feel atrialfibrillation, so he is never completely certain when he is in sinus or atrial fib. Here is his ECG: Atrial Fib with a Ventricular Response of about 66. He immediately completely recovered.
Interpreting the waves and detecting abnormalities: Typically, the heart conducts electricity in a pathway starting in the sinoatrial node (SA), our heart’s “natural pacemaker”, located in the wall of the right atrium. Sinus bradycardia – sinus rhythm below 60 bpm is a sinus bradycardia.
Her Apple Watch suddenly told her that she is in atrialfibrillation. Patients with healthy AV nodes who are not on AV nodal blockers and who are not hyperkalemic should have a rapid ventricular response if they have paroxysmal Atrialfibrillation. Baseline bradycardia in endurance athletes limits the use of ß-blockers.
The aim of this study is to investigate the usefulness of an implantable loop recorder (ILR) for arrhythmia detection including atrialfibrillation (AF) in HFnon-rEF patients after discharge. Methods and analysis This is a multicentre single arm study to evaluate the usefulness of ILR for detecting arrhythmia.
Complete left bundle branch block (CLBBB)-like QRS morphology of right ventricular pacing at pacemaker implantation satisfying the American Heart Association/American College of Cardiology Foundation/Heart Rhythm Society criteria of CLBBB was associated with development of pacing induced cardiomyopathy.
She previously had Atrialfibrillation with LBBB. This shows atrialfibrillation. The fact that the response is regular proves that the atrialfibrillation is NOT conducting. When atrial fib conducts, the ventricular rate must always be irregular. She had a permanent pacemaker implanted.
AtrialFibrillationAtrialfibrillation causes irregular heartbeat, and the heart's normal blood supply is affected. Since atrialfibrillation can also be intermittent, such patients should continuously monitor their heart activity while performing daily activities with a portable ECG device.
PVCs N ot generally considered abnormal ECG findings: Isolated PAC, First Degree AV Block, Sinus bradycardia at a rate of 35-45, and Nonspecific ST-T abnormalities (even if different from a previous ECG). Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful.
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. 2:34 PM, following right heart catheterization She then went into atrialfibrillation with complete heart block and junctional escape rhythm prompting placement of transvenous pacemaker.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content