This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
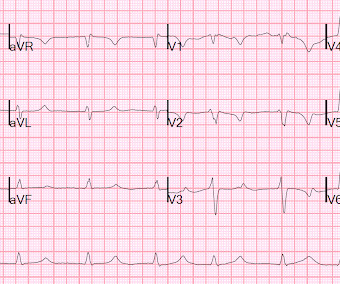
PMH: Known paroxysmal Atrial fib. He is usually is in sinus rhythm as far as he knows, but he cannot subjectively feel atrialfibrillation, so he is never completely certain when he is in sinus or atrial fib. Here is his ECG: Atrial Fib with a Ventricular Response of about 66. He immediately completely recovered.
Written by Pendell Meyers First try to interpret this ECG with no clinical context: The ECG shows an irregularly irregular rhythm, therefore almost certainly atrialfibrillation. After an initially narrow QRS, there is a very large abnormal extra wave at the end of the QRS complex. Is there a long QT? How would you manage this patient?
Due to bradycardia, a 12-lead ECG was obtained: There is atrialfibrillation at a rate of 54. But because of bradycardia, a 12-lead was obtained, which gave the critical diagnosis. Slow atrialfibrillation implies an sick AV node, or one affected by electrolytes, ischemia, or medications/drugs.
Her Apple Watch suddenly told her that she is in atrialfibrillation. Patients with healthy AV nodes who are not on AV nodal blockers and who are not hyperkalemic should have a rapid ventricular response if they have paroxysmal Atrialfibrillation. Baseline bradycardia in endurance athletes limits the use of ß-blockers.
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Atrialfibrillation is also a predictor of worse outcomes in this case (Alborzi). Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ).
Remember, in diffuse subendocardial ischemia with widespread ST-depression there may b e ST-E in lead s aVR and V1. There are well formed R-waves with good voltage/amplitude which is uncommon for ischemia. The ECG does not show any signs of ischemia. True Positive ECG#2 : Also sinus rhythm. There is ST depression in V1.
She previously had Atrialfibrillation with LBBB. This shows atrialfibrillation. The fact that the response is regular proves that the atrialfibrillation is NOT conducting. When atrial fib conducts, the ventricular rate must always be irregular. There was no evidence of ischemia.
AtrialFibrillationAtrialfibrillation causes irregular heartbeat, and the heart's normal blood supply is affected. Since atrialfibrillation can also be intermittent, such patients should continuously monitor their heart activity while performing daily activities with a portable ECG device.
Osborn waves have been reported with hypercalcemia, brain injury, subarachnoid hemorrhage, Brugada syndrome, cardiac arrest from VFib — and — severe, acute ischemia resulting in acute MI ( See My Comment in the November 22, 2019 post on Dr. Smith’s Blog ). Rituparna et al — as well as Chauhan and Brahma ( Int.
There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Torsades in acquired long QT is much more likely in bradycardia because the QT interval following a long pause is longer still. There is atrialfibrillation. mEq/L: The STE is resolved.
Evidence of acute ischemia (may be subtle) vii. PVCs N ot generally considered abnormal ECG findings: Isolated PAC, First Degree AV Block, Sinus bradycardia at a rate of 35-45, and Nonspecific ST-T abnormalities (even if different from a previous ECG). Left BBB vi. Pathologic Q-waves viii. LVH or RV d. Abnormal but less worrisome: i.
This ECG shows a sinus bradycardia with a normal conduction pattern (normal PR, normal QRS, and normal QTc), normal axis, normal R-wave progression, normal voltages. Hypothermia can also produce bradycardia and J waves, with a pseudo-STEMI pattern. ECG met STEMI criteria and was labeled STEMI by computer interpretation.
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. It is possible there is microvascular dysfunction producing residual transmural ischemia. He told the patient this horrible news. The other point in favor of RCA is junctional rhythm.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content