This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BMI, body mass index; eGFR, estimated glomerular filtration rate; NYHA, New York Heart Association. 1.38), a diagnosis of atrialfibrillation (HR 1.24, 95% CI 1.10–1.39), 1.29), diabetes mellitus (HR 1.15, 95% CI 1.04–1.27) m 2 (hazard ratio [HR] 1.75, 95% confidence interval [CI] 1.34–2.27), m 2 (HR 1.51, 95% CI 1.37–1.66),
Share Cardiovascular Disease Those in the ‘Ideal’ category were 55% less likely to develop diseases of the circulatory system, including: Heart Disease Stroke Heart Failure AtrialFibrillation For each 10-point increment in lifestyle score, there was a proportionate 20% reduction in these conditions combined.
Abstract Introduction During atrialfibrillation ablation (AFA), achievement of first pass isolation (FPI) reflects effective lesion formation and predicts long-term freedom from arrhythmia recurrence. Multivariate analysis showed that BMI > 30 (OR 0.78 [0.64–0.96]) 0.96]) and LA volume (OR per mL increase = 1.00 [0.99–1.00])
Propensity score-matched analysis (PSM) (1:1) was performed with matching for age, gender, race, BMI, hypertension, diabetes mellitus, chronic kidney disease, hemoglobin level, low-density lipid (LDL) level, left ventricular ejection fraction, and various drugs including ACEi, ARBi, ARNI, beta-blockers, and diuretics.
Then identified clusters are predicted and tested in the learning set to evaluate their association with outcomes. Finally, the reproducibility of the results of cluster analysis is tested in an external cohort (validation set).
17.4]) and was also more likely to have diabetes mellitus, hyperlipidemia, chronic lung disease, chronic kidney disease, chronic liver disease, BMI ≥ 25, anemia, metastatic cancer, and atrialfibrillation. The hemophilia cohort was slightly older (63.2[16.8]
Outcomes were 1 year hospital readmission rates by all-cause and due to repeat stroke.Results:Patients in the intervention group and control group were similar in age, BMI, race, smoking status, as well as rates of hypertension, diabetes, hyperlipidemia, atrialfibrillation, and history of prior stroke, with the exception of discharge rate to skilled (..)
Participants with LVI were significantly older, male, Black, had higher BMI, and lower HDL. Participants with LVI were more likely to have diabetes, tobacco use, and atrialfibrillation (24% versus 14%, p<0.001).
The mean BMI was 27.9 One patient had diabetes, 8 had hyperlipidemia, and 9 had hypertension. Only one patient had paroxysmal atrialfibrillation, with a CHA2DS2-VASc score of 0. Of these, 9 (64%) were female with a mean age of 59.6, and 5 (36%) were male with a mean age of 55.4. kg/m2, with 4 classified as obese.
Objective While greater body mass index (BMI) is associated with increased risk of developing atrialfibrillation (AF), the impact of BMI on outcomes in newly diagnosed AF is unclear. The study population comprised 40 482 participants: 703 underweight (BMI <18.5 kg/m 2 ), 13 095 normal (BMI=18.5–24.9
The lower part of the figure shows the risk of mortality according to continuous body mass index (BMI) ( left panel ) and waist-to-height ratio (WHtR) ( right panel ). Compared to a BMI 18.524.9kg/m 2 , a BMI <18.5kg/m 2 ( n =24) was associated with a numerically, but not a significantly, higher risk of all-cause and cardiovascular death.
The primary endpoint was MACEs, which represented a composite event of all-cause death, stroke, systemic embolism, and massive hemorrhage.Results:The 2,182 patients were divided into two groups: LVEDD>60mm group (n=370) and LVEDD ≤60 mm group (n=1812).
Getty Images milla1cf Wed, 06/26/2024 - 18:59 June 26, 2024 — Semaglutide , a medication initially developed for type 2 diabetes and obesity, significantly improves symptoms in men and women with a common type of heart failure that has had few therapeutic options. It also lowered their systolic blood pressure and waist circumference.
Cohorts were matched on age, sex, diabetes, atrialfibrillation, and hypertension. The US cohort had greater ethno-racial heterogenity, higher BMI, and higher NIHSS on admission. The NOR cohort had a significantly higher proportion of previous/current smokers and a higher prevalence of hypercholesterolemia.
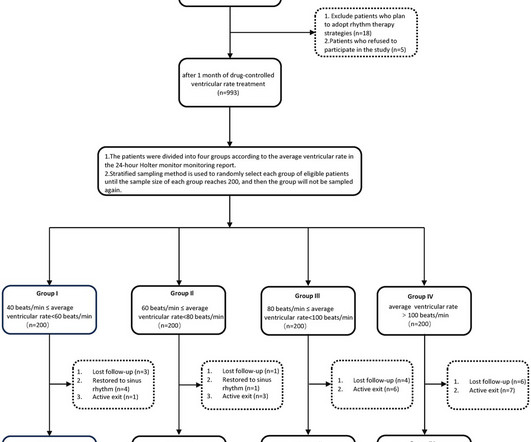
Further regression analysis indicated that body mass index (BMI) might be related to changes in LAD. However, the optimal range for ventricular rate control remains unclear. Additionally, the use of digoxin could affect changes in left ventricular ejection fraction.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content