This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In addition, abelacimab consistently reduced bleeding risk in patients 75 years of age and older regardless of renal function, body mass index (BMI), and the use of concomitant antiplatelet therapy. Patients with atrialfibrillation, particularly older patients, are frequently at a high risk of bleeding.
The TyG-BMI index, which is a reliable indicator of insulin resistance (IR), has been found to have a significant correlation with the occurrence of cardiovascular events. However, there still lacks study on t.
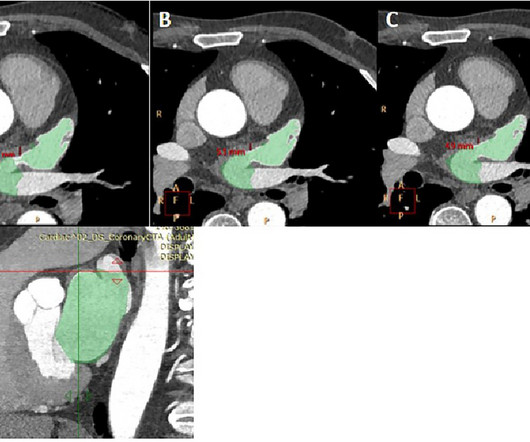
IntroductionEpicardial adipose tissue (EAT) is involved in cardiac inflammatory responses and has been associated with both atrialfibrillation (AF) and rheumatoid arthritis (RA). The volume of EAT or EAT/BMI ratio was similar between the patients with RA and no AF and those without both RA and AF.
Background Catheter ablation (CA) for symptomatic atrialfibrillation (AF) offers the best outcomes for patients. Results Our patient cohort was older, with higher BMI, greater CHA2DS2-VASc scores, and larger left atrial sizes compared to similar previously published cohorts, while gender balance and other characteristics were similar.
ABSTRACT Introduction Catheter ablation of persistent atrialfibrillation yields sub-optimal success rates partly due to the considerable heterogeneity within the patient population. Methods We studied all patients who underwent catheter ablation of persistent atrialfibrillation in the DECAAF II trial.
It incorporates age, body mass index (BMI), and atrialfibrillation to aid in the diagnosis of HFpEF. The newly developed HFpEF-ABA score model estimates the probability of HFpEF in individual patients based on three simple clinical variables: age, BMI, and atrialfibrillation.
Optimal NT-proBNP cut points for HFpEF rule out (optimizing sensitivity) and rule in (optimizing specificity) were derived and tested, stratified by obesity and atrialfibrillation. Current consensus age- and BMI-stratified rule-in thresholds demonstrated only 65% specificity (95% CI, 57%72%).
Limited data indicate an elevated risk of atrialfibrillation (AF) after neoadjuvant chemoradiation in esophageal cancer however the role of AF as an independent predictor of outcomes post-esophagectomy remains under-studied. Circulation, Volume 150, Issue Suppl_1 , Page A4142376-A4142376, November 12, 2024.
Previous studies have shown that a higher BMI is associated with AF recurrence after AF ablation using conventional thermal ablative modalities, such as radiofrequency (RF) or cryotherapy (Cryo).
BMI, body mass index; eGFR, estimated glomerular filtration rate; NYHA, New York Heart Association. 1.38), a diagnosis of atrialfibrillation (HR 1.24, 95% CI 1.10–1.39), Discontinuation and reinitiation of mineralocorticoid receptor antagonists (MRA) in patients with heart failure and reduced ejection fraction (HFrEF).
Abstract Introduction Obesity is implicated in adverse atrial remodeling and worse outcomes in patients with atrialfibrillation. The objective of this study is to assess the effect of body mass index (BMI) on ablation-induced scar formation on late gadolinium enhancement cardiac magnetic resonance imaging (LGE-CMR).
These results were successfully validated internally and externally.Conclusions:NLR, MPV, BMI and AF were independent risk factors and predictors of ENDi. The area under the curve of the prediction model constructed from the above four factors was 0.981 (95% CI 0.961-1.000) and the calibration curve was close to the ideal diagonal line.
Abstract Introduction During atrialfibrillation ablation (AFA), achievement of first pass isolation (FPI) reflects effective lesion formation and predicts long-term freedom from arrhythmia recurrence. Multivariate analysis showed that BMI > 30 (OR 0.78 [0.64–0.96]) 0.96]) and LA volume (OR per mL increase = 1.00 [0.99–1.00])
Propensity score-matched analysis (PSM) (1:1) was performed with matching for age, gender, race, BMI, hypertension, diabetes mellitus, chronic kidney disease, hemoglobin level, low-density lipid (LDL) level, left ventricular ejection fraction, and various drugs including ACEi, ARBi, ARNI, beta-blockers, and diuretics.
17.4]) and was also more likely to have diabetes mellitus, hyperlipidemia, chronic lung disease, chronic kidney disease, chronic liver disease, BMI ≥ 25, anemia, metastatic cancer, and atrialfibrillation. The hemophilia cohort was slightly older (63.2[16.8]
Individuals with FXai prescriptions for a therapeutic indication such as venous thromboembolism, atrialfibrillation (AF), and/or non-mechanical cardiac-valve replacement, were included. There is a paucity of accurate national incidence rate data on ICH, fatal ICH and ICH sub-types in patients on FXai anticoagulants (e.g.
Outcomes were 1 year hospital readmission rates by all-cause and due to repeat stroke.Results:Patients in the intervention group and control group were similar in age, BMI, race, smoking status, as well as rates of hypertension, diabetes, hyperlipidemia, atrialfibrillation, and history of prior stroke, with the exception of discharge rate to skilled (..)
Participants with LVI were significantly older, male, Black, had higher BMI, and lower HDL. Participants with LVI were more likely to have diabetes, tobacco use, and atrialfibrillation (24% versus 14%, p<0.001). There were a total of 18 ischemic stroke events among those with LVI (6%) and 65 among those without LVI (3%).
The mean BMI was 27.9 Only one patient had paroxysmal atrialfibrillation, with a CHA2DS2-VASc score of 0. Echocardiography revealed structurally normal hearts with a mean left ventricular ejection fraction of 61% and a mean left atrial volume index of 24.8 Of these, 9 (64%) were female with a mean age of 59.6,
Each outcome was examined across BMI and BW. Because few patients had a BMI <18.5 kg/m2(n=598), the primary analyses were restricted to those with a BMI ≥18.5 RESULTS:Among 58 464 patients, the median BMI was 28.3 Because few patients had a BMI <18.5 interquartile range, 25.2–32.2)
BMI, body mass index; LVEF, left ventricular ejection fraction; NT-proBNP, N-terminal pro-B-type natriuretic peptide. The beneficial effects of finerenone in patients with heart failure (HF) and mildly reduced or preserved ejection fraction were consistent, regardless of a history of chronic obstructive pulmonary disease (COPD) status.
Objective While greater body mass index (BMI) is associated with increased risk of developing atrialfibrillation (AF), the impact of BMI on outcomes in newly diagnosed AF is unclear. The study population comprised 40 482 participants: 703 underweight (BMI <18.5 kg/m 2 ), 13 095 normal (BMI=18.5–24.9
Semaglutide-mediated improvements in HF-related symptoms and physical limitations were consistent in both male and female participants across key subgroups including age and BMI. It also lowered their systolic blood pressure and waist circumference.
Then identified clusters are predicted and tested in the learning set to evaluate their association with outcomes. Finally, the reproducibility of the results of cluster analysis is tested in an external cohort (validation set). The derived algorithm was applied in the COMMANDER-HF trial ( n =5022) for external validation.
Cohorts were matched on age, sex, diabetes, atrialfibrillation, and hypertension. The US cohort had greater ethno-racial heterogenity, higher BMI, and higher NIHSS on admission. The NOR cohort had a significantly higher proportion of previous/current smokers and a higher prevalence of hypercholesterolemia.
Share Cardiovascular Disease Those in the ‘Ideal’ category were 55% less likely to develop diseases of the circulatory system, including: Heart Disease Stroke Heart Failure AtrialFibrillation For each 10-point increment in lifestyle score, there was a proportionate 20% reduction in these conditions combined.
The primary endpoint was MACEs, which represented a composite event of all-cause death, stroke, systemic embolism, and massive hemorrhage.Results:The 2,182 patients were divided into two groups: LVEDD>60mm group (n=370) and LVEDD ≤60 mm group (n=1812).
The lower part of the figure shows the risk of mortality according to continuous body mass index (BMI) ( left panel ) and waist-to-height ratio (WHtR) ( right panel ). Compared to a BMI 18.524.9kg/m 2 , a BMI <18.5kg/m 2 ( n =24) was associated with a numerically, but not a significantly, higher risk of all-cause and cardiovascular death.
Age, BMI, hypertension, CHA2DS-VASC score, neutrophil to lymphocyte ratio (NLR), LAA volume, LA volume, the myocardial thickness at the junction of LAA and LA, the area, circumference, short diameter, and long diameter of the LAA opening, were significantly different between the AF group and the control group (P<0.05).
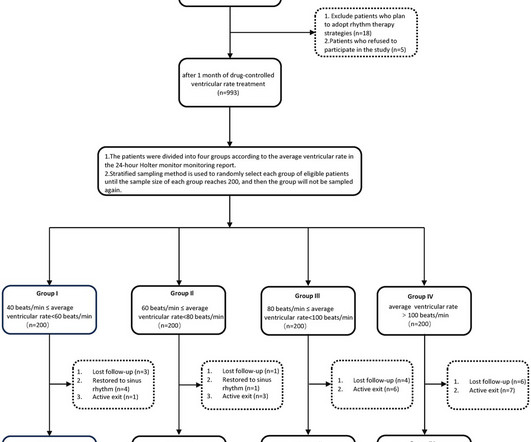
Further regression analysis indicated that body mass index (BMI) might be related to changes in LAD. However, the optimal range for ventricular rate control remains unclear. Specifically, the severity of cardiac remodeling, including LVEDD, LAD, LVEF, and mitral regurgitation, showed the following trend: Group II
ABSTRACT Introduction Epicardial adipose tissue (EAT) is often associated with atrial fibrosis, and both can provide the substrate for atrialfibrillation (AF). However, most AF patients have no evidence of left atrial (LA) fibrosis based on bipolar voltage mapping. cm, p <0.001) and higher right atrial EAT (7.3
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content