This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
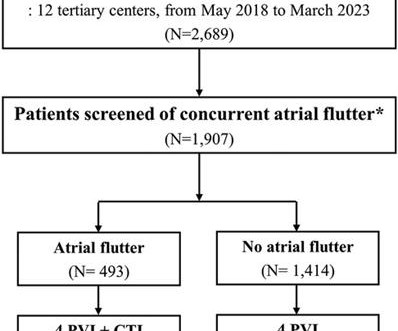
Typical atrialflutter commonly occurs in patients with atrialfibrillation (AF). Limited information exists regarding the effects of concurrent atrialflutter on the long-term outcomes of rhythm control. Patients who were screened for typical atrialflutter were included in the analysis ( n = 1,907).
male with pertinent past medical history including Atrialfibrillation, atrialflutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Description : Regular Wide Complex Tachycardia at a rate of about 160.
The trial will evaluate the outcomes of therapy provided with the FARAPULSE PFA System versus AADs, including device-or procedure-related adverse events, the rates of freedom from AF, atrialflutter, or atrialtachycardia, as well as AF burden – a measurement of the amount of AF an individual experiences. Circulation.
When atrialfibrillation (AF) begins, it can start with a single focus, degenerating to multiple wavelets, and it spreads throughout the entire surface area of both atria. A fibrillatory wave that occurs at a rate of more than 600 beats per minute can cause fatigue in the long run, leading to atrial dilation.
Wild-type transthyretin amyloid cardiomyopathy (ATTRwt-CM) is often accompanied by atrialfibrillation (AF), atrialflutter (AFL), and atrialtachycardia (AT), which are difficult to control because beta-blockers and antiarrhythmic drugs can worsen heart failure (HF).
She also has a hx of paroxysmal atrialfibrillation and is on oral anticoagulant treatment. She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. The ECG was interpreted as showing atrialflutter with 2:1 conduction. The ECG below was recorded. What is your assessment?
There is a regular wide complex tachycardia. A fully upright P-wave is typical atrial activity of atrialflutter as seen in V1. See these example cases of upright P-waves: Case Continued Thus, I was all but certain that this was atrialflutter. If it is flutter, it will reveal the underlying flutter waves.
Primary endpoint was the incidence of patients with new onset supraventricular arrhythmia (AF, atrialflutter or any supraventricular tachycardia) lasting >30s, post PFO closure.ResultsA total of 59 patients met the inclusion criteria.
Here is the computer interpretation: ATRIALFIBRILLATION WITH RAPID VENTRICULAR RESPONSE WITH ABERRANT CONDUCTION OR VENTRICULAR PREMATURE COMPLEXES LEFT AXIS DEVIATION [QRS AXIS beyone -30] NONSPECIFIC ST and T-WAVE ABNORMALITY The over-reading physician confirmed this diagnosis, which is incorrect. It is not atrialfibrillation.
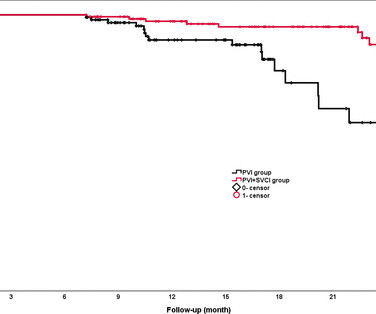
Background The value of empirical superior vena cava isolation (SVCI) following pulmonary vein isolation (PVI) to improve the efficacy of radiofrequency catheter ablation (RFCA) for paroxysmal atrialfibrillation (PAF) remains controversial. RFCA was guided by quantitative AI in both groups.
Let's first consider the heart rate: with a heart rate of 194 beats/min, the heart rate is too low for atrialflutter (1:1) (except in patients who have been pre-treated with medication), and the rate would be unusually high for atrialflutter with 2:1 conduction.
Abstract Introduction Atrialfibrillation and atrialflutter originating from the donor s heart is a commonly reported complication post heart transplant. Case A 47-year-old male presented with atrialtachycardia 6 months post heart transplant.
Wide-complex tachycardia: VT or aberrant, or "other?" The patient had a history of paroxysmal atrialfibrillation and several cardioversions. A wide-complex tachycardia in an older patient must immediately suggest ventricular tachycardia. Instead, the rate of 150, plus the history of AF, suggested atrialflutter.
Initial ECG in the ED: Presenting ECG : Wide-complex tachycardia at a rate about 200. This is overwhelmingly likely to be ventricular tachycardia, even if only age and medical history are considered. Nevertheless, the widths of both the QRS complex and the RS duration are similar in both the old ECG and the tachycardia.
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? To me, it was clearly atrialflutter with 1:1 conduction. The rate of 280 is just right for atrialflutter. The waves look like atrialflutter waves, NOT like a wide ventricular complex.
BACKGROUND:Inflammation may promote atrialfibrillation (AF) recurrence after catheter ablation. Circulation: Arrhythmia and Electrophysiology, Ahead of Print. mg twice daily or placebo for 10 days. mg twice daily or placebo for 10 days. The first dose of the study drug was administered within 4 hours before ablation.
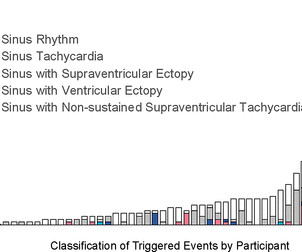
No participant demonstrated atrialfibrillation, atrialflutter, sustained supraventricular tachycardia (SVT), sustained ventricular tachycardia or infranodal atrioventricular block. Median monitoring duration was 13.2 (IQR supraventricular ectopic burden and one had a 15.4% ventricular ectopic burden.
Abstract Introduction The use of flecainide and propafenone for medical cardioversion of atrialfibrillation (AF) and atrialflutter/intra-atrial reentrant tachycardia (IART) is well-described in adults without congenital heart disease (CHD).
There is a narrow complex tachycardia at a rate of 130. ECGs: there is a regular narrow complex tachycardia still at a rate of exactly 130, with no P-waves and also no change since the prehospital ECG. Leads II and aVF appear to have flutter waves. I diagnosed atrialflutter with 2:1 conduction. Is is sinus?
FAAM ablation successfully decreased the recurrence rate of atrial tachyarrhythmia compared with conventional non-PV foci ablation. Abstract Introduction Treatment of recurrent atrialfibrillation (AF) is sometimes challenging due to non-pulmonary vein (PV) foci. The RHYTHMIA system was used to perform all the procedures.
edits by Meyers A woman in her 60s with a history of chronic atrialfibrillation on Eliquis, ESRD on hemodialysis, type-II diabetes mellitus, prior CVA, hypertension, and hyperlipidemia presented to the emergency department with multiple complaints after missing dialysis. They are flutter waves, and the rhythm is 2:1 atrialflutter.
Sinus tachycardia – sinus rhythm above 100 bpm is a sinus tachycardia. Ventricular tachycardia – more than 7 consecutive complexes originating from ventricles at a rate of > 100 bpm. Supraventricular tachycardia – more than 7 consecutive complexes of supraventricular beats at a rate of > 100 bpm.
Continue reading to learn more about this procedure, its significance in treating atrialfibrillation, and what to expect during treatment. What is AtrialFibrillation? Before diving into electrical cardioversion, we should understand atrialfibrillation (AF). What Is Cardioversion?
Although the QDOT MICRO™ Catheter was mainly designed for pulmonary vein isolation (PVI) its versatility to treat atrialfibrillation (AF) and other types of arrhythmias was recently evaluated by the FAST and FURIOUS study series and other studies and will be presented in this article.
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrialflutter with regular conduction. There are no P waves preceding the QRS complexes, and no clear flutter waves.
Atrialfibrillation, atrialtachycardia or atrialflutter with Wenckebach conduction. Although today's patient was asymptomatic with the rhythm shown in ECG #1 — having this frequent amount of PACs is of potential concern, and may increase the risk of developing atrialfibrillation.
AccurECG provides automated heart rate measurements, supraventricular and ventricular ectopic beat detection, and automated interpretation for 13 different arrhythmias such as atrialfibrillation, atrialflutter, and ventricular tachycardia.
The rhythm differential for narrow, regular, and tachycardic is sinus rhythm, SVT (encompassing AVNRT, AVRT, atrial tach, etc), and atrialflutter (another supraventricular rhythm which is usually considered separately from SVTs). Therefore this patient is either in some form of SVT or atrialflutter.
Here is his 12-lead ECG: The computer reads supraventricular tachycardia. It is atrialflutter with 2:1 conduction. There are clear flutter waves in lead II across the bottom. Adenosine simply blocks the AV node so that there is no QRS to hide the flutter waves, and they become obvious. What is it?
How can the Bix Rule help distinguish AtrialFlutter from SVT? Why is amiodarone contraindicated in patients with WPW associated with atrialfibrillation? What are the important differences in the approach and treatment of atrialfibrillation vs. atrialflutter? and many more.
ABSTRACT Introduction The safety and efficacy of paroxysmal atrialfibrillation (PAF) ablation with the HELIOSTAR multielectrode radiofrequency (RF) balloon catheter have been demonstrated in European studies; data from elsewhere are lacking. Central Illustration. Image is courtesy of Biosense Webster, Inc., All rights reserved.
Case summary A 51-year-old woman with a 36-year history of intermittent palpitations was admitted due to hemodynamically stable ventricular tachycardia (VT). She denied any family history of cardiovascular disease or sudden death.
a global leader in cardiac arrhythmia treatment and part of Johnson & Johnson MedTech , today announced European CE mark approval of the VARIPULSE Platform for the treatment of symptomatic drug refractory recurrent paroxysmal atrialfibrillation ( AF ) using pulsed field ablation (PFA). AtrialFibrillation. Circulation.
Abstract Background Dofetilide is a class III antiarrhythmic agent approved for the treatment of atrialfibrillation and atrialflutter. Given the efficacy of other class III agents, it has been used off-label for the treatment of premature ventricular complexes (PVCs) and ventricular tachycardias (VTs).
Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. There is a large peaked P-wave in lead II (right atrial enlargement) There is left axis deviation consistent with left anterior fascicular block. See my quick review of atrialtachycardia below) The tachycardia spontaneously resolved.
Procedures were most commonly for atrialfibrillation (52.4%), atrialflutter (10.9%), and atrioventricular nodal re-entrant tachycardia (10.1%). Results 1089 patients were included: MC 718 (65.9%); Fo8 HT 105 (9.6%); Fo8 MOD 266 (24.4%). 01; minor: MC 16.5%, Fo8 HT 12.0%, Fo8 MOD 7.4%, p =.002).
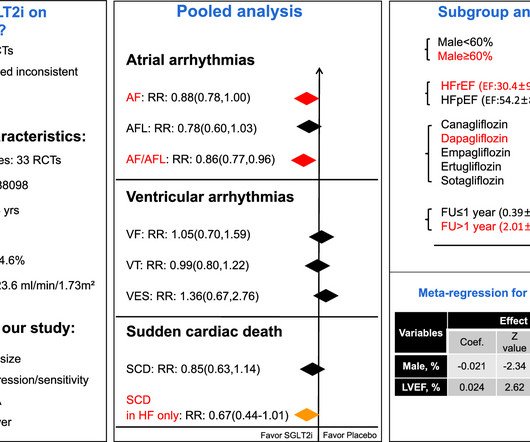
The effects of SGLT2i on atrialfibrillation(AF), atrialflutter(AFL), composite AF/AFL, ventricular fibrillation(VF), ventricular tachycardia(VT), ventricular extrasystoles(VES), sudden cardiac death(SCD) and composite VF/VT/SCD were evaluated. RCTs comparing SGLT2i with placebo were included.
Additionally, the patient had no other apparent reason to have sinus tachycardia (such as volume depletion, bleeding, fever). So the most likely rhythm in ECG 1 is ectopic atrialtachycardia. Therefore the first part of ECG 1 shows ectopic atrialtachycardia with biventricular pacing. Point 1: What is PVARP?
ABSTRACT Introduction Freedom from recurrences of atrial tachyarrhythmia (ATA) is suboptimal after pulmonary vein isolation (PVI) in patients with persistent atrialfibrillation (PsAF).
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Most physicians will automatically be worried about these symptoms. The tracings were considered abnormal in the following cases: 1.
Figure-1: While at first glance the rhythm in Figure-1 might be mistaken for sinus tachycardia in fact, this is not the rhythm. Instead there is 2:1 atrial activity that is best seen in lead V1 ( See Figure-2 ). This is the "Bix Rule" See Pearl #1 in Dr. Figure-2: Colored arrows highlight flutter waves , with 2:1 AV conduction.
ABSTRACT Typical atrialflutter (AFL), defined as cavotricuspid isthmus (CTI)-dependent macro-re-entrant atrialtachycardia, often causes debilitating symptoms, and is associated with increased incidence of atrialfibrillation, stroke, heart failure, and death.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content