This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Patients in the study will be randomized to undergo pulmonary vein isolation (PVI) and left atrial posterior wall ablation using the FARAPULSE PFA System, or receive AAD treatment, and followed for three years. The randomized AVANT GUARD trial will enroll more than 500 patients diagnosed with persistent AF at up to 75 sites globally.
Both atria develop from a combination of the primitive atrium, sinus venous, and pulmonary veins.It When atrialfibrillation (AF) begins, it can start with a single focus, degenerating to multiple wavelets, and it spreads throughout the entire surface area of both atria. We know atrialflutters can be confined to one atrium.
A significant proportion of patients with isolated atrialflutter (AFL) will develop atrialfibrillation (AF) following cavotricuspid isthmus (CTI) ablation.
male with pertinent past medical history including Atrialfibrillation, atrialflutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Bedside ultrasound showed volume depletion and no pulmonary edema.
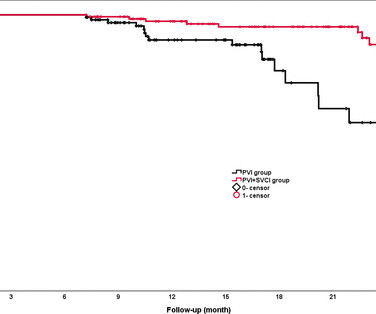
Background The value of empirical superior vena cava isolation (SVCI) following pulmonary vein isolation (PVI) to improve the efficacy of radiofrequency catheter ablation (RFCA) for paroxysmal atrialfibrillation (PAF) remains controversial. RFCA was guided by quantitative AI in both groups.
A company statement reported that its PFA System is indicated for the isolation of pulmonary veins in the treatment of drug-refractory, recurrent, symptomatic, paroxysmal (i.e., intermittent) atrialfibrillation (AF) and is a unique new alternative to standard-of-care thermal ablation treatment.
Complete and durable block across the left atrial (LA) roof can be integral to ablation of persistent atrialfibrillation (AF) and atypical atrialflutter (AFl). The right pulmonary artery (RPA) is in close proximity to the LA roof, and may provide a vantage for epicardial LA roof mapping and ablation.
Here is the computer interpretation: ATRIALFIBRILLATION WITH RAPID VENTRICULAR RESPONSE WITH ABERRANT CONDUCTION OR VENTRICULAR PREMATURE COMPLEXES LEFT AXIS DEVIATION [QRS AXIS beyone -30] NONSPECIFIC ST and T-WAVE ABNORMALITY The over-reading physician confirmed this diagnosis, which is incorrect. It is not atrialfibrillation.
It is atrialflutter with 2:1 conduction. There are clear flutter waves in lead II across the bottom. In V1, there are upright waves that appear to be P-waves but are not: they are atrial waves and it is typical for atrialflutter waves to be upright in V1, whereas sinus P-waves are biphasic in V1.
Pulmonary vein isolation (PVI) remains the cornerstone of atrialfibrillation (AF) ablation. In patients with more advanced AF subtypes, atypical atrialflutter, and extensive atrial myopathy, additional linear ablation is often required; however, durable block of these remains challenging.
FAAM ablation successfully decreased the recurrence rate of atrial tachyarrhythmia compared with conventional non-PV foci ablation. Abstract Introduction Treatment of recurrent atrialfibrillation (AF) is sometimes challenging due to non-pulmonary vein (PV) foci. The RHYTHMIA system was used to perform all the procedures.
a global leader in cardiac arrhythmia treatment and part of Johnson & Johnson MedTech , today announced European CE mark approval of the VARIPULSE Platform for the treatment of symptomatic drug refractory recurrent paroxysmal atrialfibrillation ( AF ) using pulsed field ablation (PFA). AtrialFibrillation. Circulation.
Although the QDOT MICRO™ Catheter was mainly designed for pulmonary vein isolation (PVI) its versatility to treat atrialfibrillation (AF) and other types of arrhythmias was recently evaluated by the FAST and FURIOUS study series and other studies and will be presented in this article.
Re-entrant tachycardias (atrialflutter, PSVT, AVRT, VT) have constant regular heart rates, whereas sinus tachycardia will usually gradually change rate with differing conditions (for instance, after infusion of fluid and BP increase, sinus tach rate might decrease from 130 to 125, for instance). So there is a re-entrant rhythm.
ABSTRACT Introduction The safety and efficacy of paroxysmal atrialfibrillation (PAF) ablation with the HELIOSTAR multielectrode radiofrequency (RF) balloon catheter have been demonstrated in European studies; data from elsewhere are lacking. Central Illustration. Image is courtesy of Biosense Webster, Inc., All rights reserved.
ABSTRACT Introduction Freedom from recurrences of atrial tachyarrhythmia (ATA) is suboptimal after pulmonary vein isolation (PVI) in patients with persistent atrialfibrillation (PsAF).
The PulseSelect Pulsed Field Ablation System, which was FDA approved in December 2023, offers physicians a safe, single-shot solution for pulmonary vein isolation (PVI) while the Affera Sphere-9 catheter enables physician treatment flexibility with its wide area focal design and 9mm lattice tip that can used with an 8.5Fr sheath.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content