This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Abstract: The mechanism of in-stent restenosis (ISR) remains elusive, and in-stent neoatherosclerosis (ISNA) may hold siginificant pathophysiological implications. Nevertheless, the correlation between ISNA and the progression of untreated coronary segments affected by native atherosclerosis remains incompletely investigated.
IntroductionDrug‐eluting stent (DES) use in symptomatic intracranial atherosclerosis disease (ICAD) has been described in the literature using different guiding and distal access catheters. Decision was made to deploy a drug eluting stent into the stenosed M1 segment.
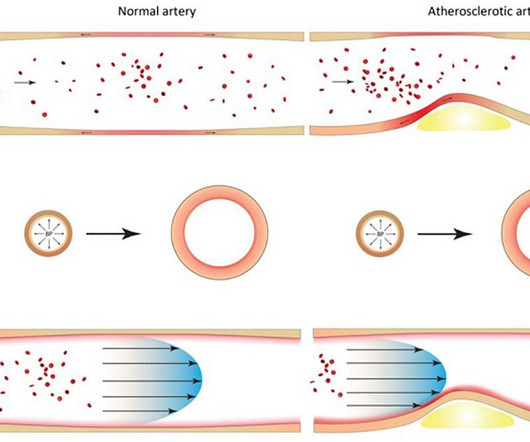
Although the entire vascular bed is constantly exposed to the same risk factors, atherosclerosis manifests a distinct intra-individual pattern in localization and progression within the arterial vascular bed.
IntroductionVertebral artery stenting represents a viable option in treating symptomatic vertebral artery atherosclerotic stenosis. We included articles reporting patients > 18 years old with symptomatic extracranial vertebral artery stenoses due to atherosclerosis treated with stenting (with or without angioplasty).
3) Rescue stenting (RS) in these patients has shown promising rates of recanalization and better outcomes in preliminary studies. Therefore, rescue stenting can be considered as a safe and viable option in these patients. 1, 2)These patients are also more likely to experience poor functional outcomes. (3)
BACKGROUNDRescue intracranial stenting (RICS) is increasingly recognized as a potentially effective rescue strategy following failed mechanical thrombectomy (MT) for large vessel occlusion due to intracranial atherosclerosis, but populationlevel data on contemporary patterns of RICS utilization in MT are lacking. had codes for MT.
Coronary heart disease is a narrowing or obstruction of the vascular cavity caused by atherosclerosis of the coronary arteries, which leads to myocardial ischemia and hypoxia. At present, percutaneous coronary intervention (PCI) is an effective treatment for coronary atherosclerotic heart disease.
Introduction:Current guidelines do not support the use of stenting for severe symptomatic intracranial atherosclerotic disease (ICAD) over maximal medical therapy (MMT) as first line treatment. Periprocedural stroke was defined as <7d from stent placement. Stroke, Volume 56, Issue Suppl_1 , Page A41-A41, February 1, 2025.
The longstanding benefits of percutaneous angioplasty and stenting in coronary artery disease, where atherosclerosis is the overarching cause in nearly all cases, provided a compelling rationale for exploring similar interventions in intracranial atherosclerotic stenosis.
For decades, the ACAS (Asymptomatic Carotid Atherosclerosis Study) and ACST (Asymptomatic Carotid Surgery Trial) trials provided most of the evidence supporting endarterectomy for patients with asymptomatic high-grade stenosis who were otherwise good candidates for surgery.
Background Kounis syndrome is an acute coronary syndrome (ACS) caused by allergic reactions, including coronary artery spasm (type I) caused by allergies without coronary predisposing factors, pre-existing coronary atherosclerosis, and coronary artery disease.
IntroductionIntracranial atherosclerosis‐related large vessel occlusion (ICAS‐LVO) is a common cause of failed mechanical thrombectomy (MT) in acute ischemic stroke (AIS) [1]. Treatment of ICAS‐LVO with rescue stenting and/or angioplasty has shown promising outcomes, but diagnosing ICAS‐LVO during MT can be challenging [2, 3].
IntroductionCerebrovascular disease (CVD), particularly carotid artery atherosclerosis, contributes substantially to global morbidity and mortality. The ability to precisely detect atherosclerosis is crucial, as it directly influences patient management, including decisions regarding surgical interventions.
Most respondents (86%) preferred acute treatment of ICAS‐LVO with rescue stenting (RS)±angioplasty. Stroke: Vascular and Interventional Neurology, Ahead of Print. However, in patients who achieved recanalization with a severe fixed focal stenosis, most (58%) recommended primary medical management.
The transplant renal artery lesion was intervened with a stent. Urine output gradually returned after 3 weeks, and serum creatinine level was normalized after 2 months.ConclusionsTransplant recipients commonly have atherosclerosis and hypertension, which are risk factors for arterial dissection.
IntroductionOcular ischemic syndrome (OIS) is a rare, vision‐threatening condition resulting from severe carotid artery disease secondary to severe atherosclerosis or arteritis. Given acute loss of vision likely secondary to ocular ischemic syndrome, decision was taken to proceed with rescue stenting. cases per million every year.
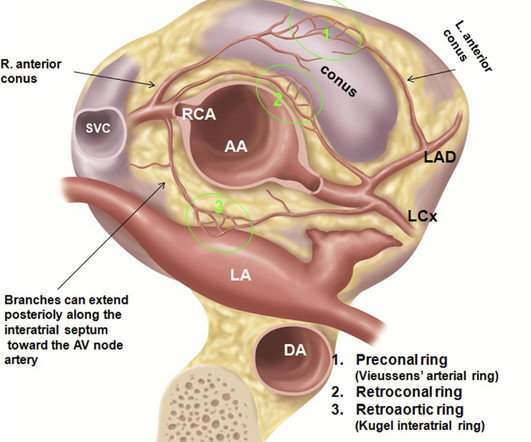
There is an area of dense white in the middle of the circle consistent with atherosclerosis. They too have dense white masses consistent with coronary atherosclerosis. This was a presumed culprit and a stent was placed. . __ Here are some Images: The red circle shows the LAD coursing down the anterior interventricular sulcus.
Importantly, all of the participants had recently undergone percutaneous coronary intervention (PCI) — a surgical procedure in which a stent is placed in a coronary artery to open up a blockage. LDL and ApoB — which play an obligate and causal role in the development of atherosclerosis — weren’t affected by exercise.
CT angiography (CTA) of the head and neck demonstrated a nearly occlusive thrombus of the distal right M2 segment MCA as well as non‐hemodynamic stenosis of the proximal right ICA with possible underlying sidewall filling defect‐appearing lesion concerning for a posterior wall thrombus without underlying atherosclerosis at the bulb or otherwise.
carotid stenting) or systemic anticoagulation, hemorrhagic complications, and whom received at least one antiplatelet agent upon discharge. Major DAPT determinants were premorbid SAPT and large-artery atherosclerosis. Independent determinants of DAPT prescription are shown in Table 1.Conclusion:DAPT
Considering their multidirectional effect on atherosclerosis, new inflammatory biomarkers integrating various leukocyte subgroups have been proposed to calculate the systemic inflammatory response index (SIRI) and systemic inflammatory index (SII).Aim:The All patients had interventional PCI with balloon and stent insertion.
We assessed the clinical outcomes of endovascular treatment in acute large vessel occlusion (LVO) strokes caused by ICAD and compared them with large vessel occlusion strokes not associated with intracranial atherosclerosis (non-ICAD LVO).Methods:Our
Ostial Athero-sclerosis( Rare, but status of other areas of coronary artery will usually reveal evidence for atherosclerosis) True confirmation, is possible only during surgery , ie visulaing the absence of left coronary ostia. Aorto arteritis 3.Ostial In reality, there could be thousands of asymptomatic ones in the public domain.
Repeat CTA head and neck demonstrated multifocal intracranial atherosclerosis with marked stenosis of the left V4 segment. However, marked stenosis at V2 appeared to be owed to external compression from facet arthrosis rather than atherosclerosis. He also had moderate stenosis of the right V4 segment.
It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chest pain. 4] CT revealed no dissection but extensive coronary atherosclerosis. In a study last year, 14.4% of those who presented within two hours and 18.1% of those with posterior MI.[4]
IntroductionIntracranial atherosclerosis (ICAS) is a leading global cause of stroke. The role of intracranial stenting in ICAS remains uncertain. The VISSIT trial found an increased 12‐month risk of TIA/CVA in the same territory, as well as an increased 30‐day risk of any TIA/CVA, when a stenting was used in patients with ICAS [2].
A higher proportion of failure cases were due to large artery atherosclerosis (30.6% Stent‐retrieval alone (SR) was a more common first pass technique in failed than in successful MT (14.3% Stent‐retrieval alone (SR) was a more common first pass technique in failed than in successful MT (14.3% vs 0%, p=0.039). vs 0%, p=0.001).ConclusionThis
A CT CAC scan can only identify if there is calcified atherosclerosis, where it is and to what extent. A CT CAC scan of 0 indicates no significant amount of calcified atherosclerosis. It does not imply that there is NO advanced atherosclerosis. And it matters. They are not fantastic odds, in my view.
pre-existing, stable atherosclerosis) amidst any state of global duress – to include hypertension, hypoxia, tachycardia, hypotension, sepsis, and GI bleed, for example. Advanced multi-vessel disease was found with stents deployed to the mid-LCx (80% stenosis), D1 (90% stensosis), and the pLAD (95% stenosis).
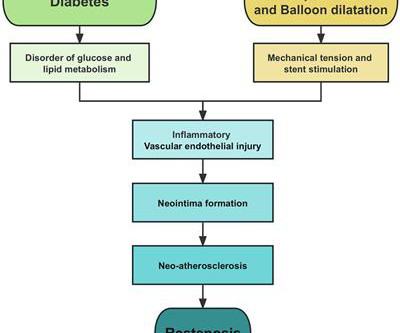
Diabetes mellitus (DM) promotes atherosclerosis, leading to increased risk for cardiovascular morbidity and mortality. These events are caused by both patient-related accelerated atherosclerotic disease progression and worse stent-related adverse clinical outcomes translating into a higher risk for repeat revascularization.
Atherosclerosis & Arterial Diseases Peripheral Artery Disease (PAD) : A blockage in your legs. Angioplasty & Stenting: Opens blocked arteries to improve blood flow. Common Vascular Conditions We Treat Some vascular diseases affect your arteries while others occur in your veins.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content