This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
There is an area of dense white in the middle of the circle consistent with atherosclerosis. They too have dense white masses consistent with coronary atherosclerosis. The cardiologist recognized that there were EKG changes, but did not take the patient for emergent catheterization because the EKG was “not meeting criteria for STEMI”.
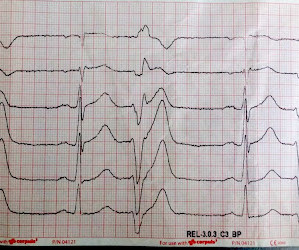
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Thus, angiography may be fairly accurate in determining lumen size, but it will not detect the “volume” of atherosclerosis present. He does have a recently diagnosed PE, and has not been taking his anticoagulation due to cost.
See "Mechanisms of acute coronary syndromes related to atherosclerosis".) STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. From Gue at al.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
Steffen writes this case: "A few weeks ago I was able to recognize a STEMI because of what I had seen on your blog." "I He had no further risk factors for atherosclerosis besides hypertension. Steffen wrote: " I remembered the ECG from your blog titled: "STEMI Seen Best in PVC, Diagnosed by Medic, Ignored by Physician" from 2013.
Considering their multidirectional effect on atherosclerosis, new inflammatory biomarkers integrating various leukocyte subgroups have been proposed to calculate the systemic inflammatory response index (SIRI) and systemic inflammatory index (SII).Aim:The The mean age of patients was 57.68 (SD= 11.19) years.
Ostial Athero-sclerosis( Rare, but status of other areas of coronary artery will usually reveal evidence for atherosclerosis) True confirmation, is possible only during surgery , ie visulaing the absence of left coronary ostia. We know, how adverse is the outcome of Left main STEMI. Syphilis 2. Aorto arteritis 3.Ostial
See "Mechanisms of acute coronary syndromes related to atherosclerosis".) STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. From Gue at al.
We have found in our study comparing inferior STEMI (manuscript in preparation) to inferior early repol several distinguishing characteristics. Nevertheless, even young people have atherosclerosis and plaque rupture. And young women have worse outcomes than other groups with STEMI because of the tendency to say, "Nah, couldn't be!"
This is a troponin I level that is almost exclusively seen in STEMI. So this is either a case of MINOCA, or a case of Type II STEMI. If the arrest had another etiology (such as old scar), and the ST elevation is due to severe shock, then it is a type II STEMI. I believe the latter (type II STEMI) is most likely.
Spontaneous coronary artery dissection Dissection of a coronary artery may occur in the context of atherosclerosis, or be iatrogennic during angiography or angioplasty. A recent study found that SCAD causes almost 20% of STEMI in young women. examined SCAD presenting as STEMI (unlike Hassan et al. A study by Hassan et al.
A "STEMI alert" was called and soon cancelled. This pattern occurs regardless of whether the cause is ACS (decreased supply) or any other cause of decreased supply or increased demand. There is a tiny hint of STE in aVL, but overall I do not think this looks like high lateral OMI. Pain lasted for approximately 45 minutes.
pre-existing, stable atherosclerosis) amidst any state of global duress – to include hypertension, hypoxia, tachycardia, hypotension, sepsis, and GI bleed, for example. STEMI was activated and the patient went to Cath on arrival. There may even be significant overlap between these factors.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content