This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
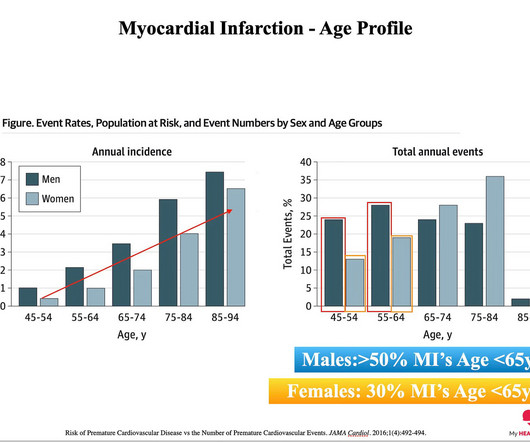
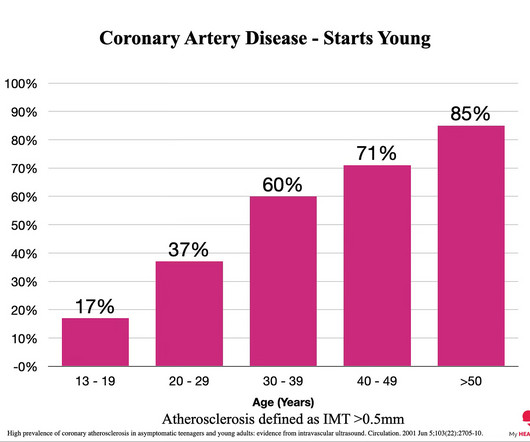
The reason: They were accumulating plaque in their coronary arteries much earlier than their peers. You can’t have a heart attack if you don’t have plaque in your coronary arteries. And plaque in your coronary arteries is the result of exposure to riskfactors over time. The answer: RiskFactors.
Aging is known to be a riskfactor for the biological changes that create the dangerous buildup of plaque in arteries called atherosclerosis, and aging also induces a buildup of memory CD8 T cells, a type of immune cell, in mice and humans.
In this 6-month randomized controlled study, twice-weekly HIIT reduced coronary plaque volume, increased aerobic fitness, and improved body composition in adults with stable heart disease, suggesting benefits for cardiovascular disease progression. Does this greater plaque presence put athletes at a greater risk of CVD events?
Metal exposure from environmental pollution is associated with increased calcium buildup in the coronary arteries at a level comparable to traditional riskfactors, according to a new study.
Although the entire vascular bed is constantly exposed to the same riskfactors, atherosclerosis manifests a distinct intra-individual pattern in localization and progression within the arterial vascular bed.
BackgroundPlaque progression (PP) is critical between subclinical atherosclerosis and plaque rupture. Intensive control of sdLDLC along with other riskfactors should be considered to mitigate PP and improve cardiovascular outcomes. Journal of the American Heart Association, Ahead of Print.
Background:Most ischemic strokes are caused by atherosclerosis. Atherosclerotic plaque formation is modulated by genetic and environmental interactions. Apolipoprotein E (ApoE) regulates lipid metabolism, and its deficiency is associated with dyslipidemia and atherosclerosis.
The complex development of atherosclerosis manifests as intimal plaque which occurs in the presence or absence of traditional riskfactors. CCTA also has the potential to de-risk clinical endpoint-based trials both financially and by enrichment of participants at higher likelihood of MACE.
Artery Damage : Hypertension damages the inner lining of your arteries, making them less elastic and more prone to plaque buildup. This condition, called atherosclerosis, narrows the arteries, restricting blood flow and increasing the risk of heart attacks and strokes.
CCR5, a chemokine receptor, has been associated with both immunosuppressive and inflammatory phenotypes, however, the possible role of CCR5 pertaining to MDSCs in the development of atherosclerosis has not been elucidated yet. Possibly this dysfunctionality contributes to the development and progression of CVD including atherosclerosis.
Lp(a) is emerging as an important, yet under-recognized, potential riskfactor for cardiovascular disease due to its ability to promote the development of plaques within artery walls, clot formation and aortic valve calcification. The development of the Tina-quant Lipoprotein (a) Gen.2 2022 Aug, 80 (9) 934946 Kronenberg F.
BackgroundThe relationship between depression and subclinical coronary atherosclerosis in asymptomatic individuals is not clear. The degree and extent of subclinical coronary atherosclerosis were evaluated by coronary computed tomographic angiography, and ≥50% diameter stenosis was defined as significant. 2.03];P=0.450).
Any atherosclerotic plaque is bad, and its presence portends a worse prognosis if modifiable riskfactors like hypertension and smoking are not addressed.
At the patient level, those with reduced CFR showed a significantly higher prevalence of diffused atherosclerosis (41% vs. 23%; P < 0.001) and higher FAI (−75.5 HU In the patient-level analysis, obstructive CAD, diffused atherosclerosis, and FAI were independently linked with CFR. Results We detected a decrease in CFR (<2.5)
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). There is an area of dense white in the middle of the circle consistent with atherosclerosis. The blue circle shows the LCx.
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. See "Mechanisms of acute coronary syndromes related to atherosclerosis".)
Background:Intracranial Atherosclerosis (ICAS) leads to stroke by perforator disease, artery to artery embolism, and impaired distal flow/perfusion. While medical treatment is likely to stabilize atherosclerotic plaques, it is unlikely to improve distal perfusion in the acute setting. The study outcome is recurrent ischemic stroke.
Compared with healthy vascular aging, arteriosclerosis and atherosclerosis clusters showed a graded positive association with cardiac troponin I quintiles, independent of traditional riskfactors.
Angiography showed a donor renal artery dissection distal to the moderately stenosed anastomosis site with calcified atherosclerotic plaque confirmed by IVUS. Our case showed that endovascular intervention can replace surgery to repair very early vascular complications such as dissection and help patients avoid high-risk operations.
Immune-mediated inflammatory diseases (IMIDs) are recognised riskfactors for accelerated atherosclerotic cardiovascular disease (CVD), particularly in younger individuals and women who lack traditional CVD riskfactors.
Coronary artery calcification (CAC) accompanies the development of advanced atherosclerosis. Nevertheless, the relationship between CAC and the susceptibility of a plaque to provoke a thrombotic event remains incompletely understood. This review summarizes the current understanding and literature on CAC.
For decades, the ACAS (Asymptomatic Carotid Atherosclerosis Study) and ACST (Asymptomatic Carotid Surgery Trial) trials provided most of the evidence supporting endarterectomy for patients with asymptomatic high-grade stenosis who were otherwise good candidates for surgery. Stroke, Ahead of Print.
The identification of a variant in theHDAC9gene as a riskfactor for large-artery atherosclerotic stroke, and subsequently coronary artery disease, has opened novel treatment pathways for stroke and more widely atherosclerotic disease. Stroke, Volume 54, Issue 12 , Page 3182-3189, December 1, 2023.
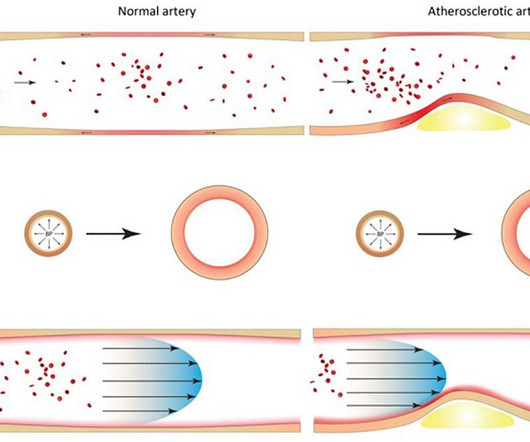
IntroductionAtherosclerosis, the hardening and narrowing of the arteries, occurs due to the buildup of plaque on the inner walls of the arteries which can result in reduced blood flow to the organs and tissues. Riskfactors such as smoking, chronic kidney disease, and aging can contribute to plaque formation.
Sustained inflammation can damage your blood vessels, leading to atherosclerosis (plaque buildup) and increasing your risk of heart attack and stroke. This can lead to chest pain (angina) and increase your risk of heart attack or stroke, especially if you already have underlying heart disease.
Introduction:Mechanical thrombectomy (MT) devices were fundamentally designed for the treatment of cardioembolic (CE) strokes despite that 10-20% of large vessel occlusions (LVO) are caused by large artery atherosclerosis (LAA), which may not respond comparably. p<0.0001), and ICA bulb plaque with high-risk features (87.9%
If the arrest was caused by acute MI due to plaque rupture, then the diagnosis is MINOCA. Here is my comment on MINOCA: "Non-obstructive coronary disease" does not necessarily imply "no plaque rupture with thrombus." They often cannot even be recognized as culprits, as fissured or ulcerated plaque. FFR can be useful.
However, CTA head and neck 4 days later demonstrated 90 percent stenosis of the mid left V2 at the C3‐4 level and a 75‐90 percent stenosis of the left mid V2 segment at the C5‐6 level (hard and soft plaque in these areas). Timely diagnosis is imperative, as decompressive surgery can be curative.
Riskfactors for cardiovascular disease Understanding the riskfactors for cardiovascular disease is crucial for maintaining optimal cardiovascular health. While some riskfactors, such as age and family history, cannot be changed, others are within our control.
While advances in treatment have reduced mortality in some regions, the atherosclerosis prevention remains challenging. This shift results from an epidemiologic transition: as infectious diseases decline, chronic conditions like atherosclerosis dominate.
No thromboembolism risks, not pleuritic, no radiation to the back. No cardiac riskfactors, no cocaine use. Nevertheless, even young people have atherosclerosis and plaque rupture. History: Onset of CP 2.5 hours prior to ED arrival. Tight and pressure, radiates to right arm, + nausea, + SOB.
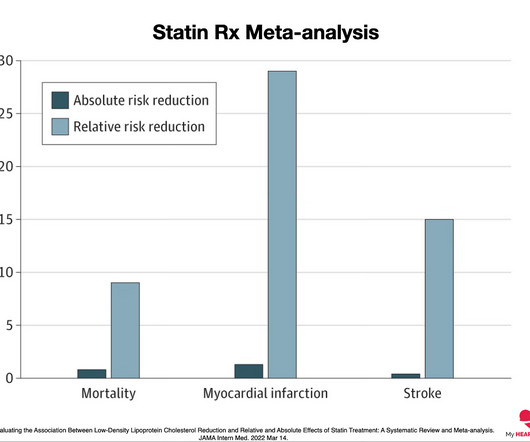
mg reduces the risk of major adverse cardiovascular events (MACE) and supports its use in the treatment of cardiovascular disease. mg)has potential to directly reduce inflammation, which plays a substantial role in the formation and progression of atherosclerotic plaque leading to heart disease, said Matthew J.
This registry will aim to provide world-wide physicians the most accurate information on coronary plaque to improve cardiovascular risk prediction and support the selection of patient-specific treatment,” said Dr. De Cecco. Márton Kolossváry (Gottsegen National Cardiovascular Center, Budapest, Hungary).
The pathology that causes heart disease (atherosclerosis) is, by definition, the abnormal retention of a cholesterol particle in the artery wall. A heart attack is when that plaque ruptures and stops blood flow down the artery. But other factors also play a role. 1 ” Good question.
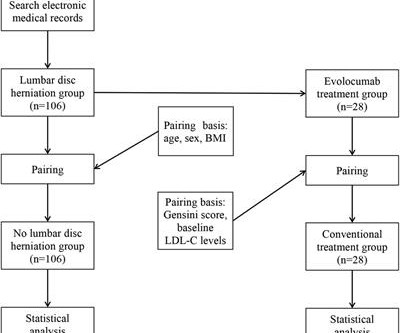
Objective Assessing the impact of lumbar disc herniation (LDH) on the plaque burden of coronary atherosclerosis is our objective. Gensini scores were calculated to assess the plaque burden of coronary. Logistic analysis was used to examine potential risk variables linked to the Gensini score.
Heart disease is the presence of plaque or atherosclerosis in the coronary arteries. Over a long enough time horizon, pretty much everyone will develop a significant amount of plaque and have a heart attack. We have very strong evidence to support the idea that the more plaque you have, the greater your risk of a heart attack 1.
Heart disease remains one of the leading causes of death worldwide, often attributed to a mix of lifestyle choices, environmental factors, and genetic predispositions. This blog explores how genetics influence heart health and whether mitigating these inherited risks is possible. Can You Prevent Heart Disease if Its in Your Genes?
When we say heart disease, what we really mean is plaque in the artery wall. This Is Known As Atherosclerosis. The fundamental cause of atherosclerosis is when a cholesterol particle crosses into the artery wall from the bloodstream, gets stuck, and sets off an inflammatory process 1. No atherosclerosis. No heart attacks.
Primordial prevention is changing the environment around you so you do not develop the riskfactors for heart disease and, by extension, do not get the disease early in life. Blood Pressure Control High blood pressure is the riskfactor associated with the greatest number of deaths worldwide. J Am Heart Assoc.
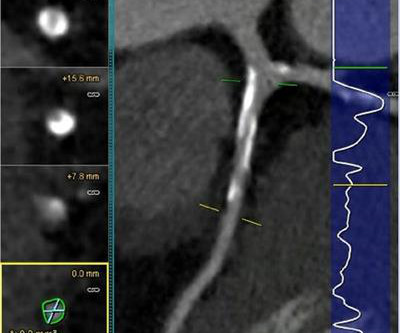
The EAS 2024 Congress (May 26-29, 2024) has concluded, providing critical insights into atherosclerosis and related vascular disease. Giovanna Liuzzo (Italy) revealed that advancements in noninvasive imaging recently allow for direct visualization of coronary atherosclerotic plaques. Here are some notable highlights: Prof.
However, most adults will start to develop advanced plaque in their coronary arteries early in life. By age 66, more than half of all females will have evidence of advanced plaque in their coronary arteries, as seen on a CT calcium score. Coronary atherosclerosis, as evidenced by an abnormal CAC score, is a measure of advanced plaque.
To understand why the answer is always ‘Now’, I want to highlight three key points and then point to the evidence that supports the idea that reducing risk early is always better. Everyone starts with no plaque in the coronary arteries, but over a long enough time frame, everyone develops plaque in their coronary arteries.
people from the general population), coronary artery calcium scores (CACS) are higher, indicating more calcification and the presence of atherosclerotic plaques. Calcified plaques are known to be more stable and less prone to rupture and lead to a heart attack. When comparing athletes to control groups (i.e., hours per week).
BackgroundCardiovascular disease (CVD) is a leading cause of death in women with systemic lupus erythematosus (SLE) due to accelerated atherosclerosis that is not predicted by established CVD risk scores. CVD risk was assessed using QRISK3 (which includes SLE diagnosis as a riskfactor) and Framingham Risk Score.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content