This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." examined SCAD presenting as STEMI (unlike Hassan et al.
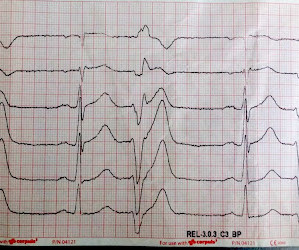
Shortly after receiving epinephrine, the patient developed new leg cramps and chestpain. The chestpain was described as sharp and radiated to both arms. During active chestpain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF.
A 20-something male presented from an outside facility with Chestpain. He came with this ECG from the outside facility, recorded 1 hour after pain onset: There is at least 2 mm of inferior ST elevation, with reciprocal ST depression in aVL, ST flattening in V4-V6, and T-wave inversion in V2. Vital signs were normal.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. He was given aspirin and sublingual nitro and the pain resolved. Thus, angiography may be fairly accurate in determining lumen size, but it will not detect the “volume” of atherosclerosis present. He was started on nitro gtt.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. Step 1 to missing posterior MI is relying on the STEMI criteria. But it is still STEMI negative. What do you think? A 15 lead ECG was done (below).
Steffen writes this case: "A few weeks ago I was able to recognize a STEMI because of what I had seen on your blog." "I I have enclosed the ECG from a 50-something year old male who complained of chestpain. He had no further risk factors for atherosclerosis besides hypertension. The rhythm is ventricular bigeminy.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content