This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
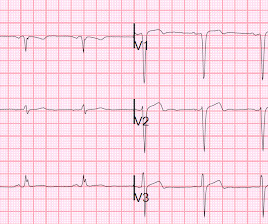
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent. So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion.
Background Hyperglycemia, characterized by elevated blood glucose levels, is frequently observed in patients with acute coronary syndrome, including ST-elevation myocardial infarction (STEMI). There are conflicting sources regarding the relationship between hyperglycemia and outcomes in STEMI patients. 3.45) and 4.47 (95% CI: 2.54–7.87),
Primary percutaneous coronary intervention (PPCI) remains the gold-standard treatment for ST-elevation myocardial infarction (STEMI). We present the case of a man in his 50s, admitted with cardiac arrest secondary to inferolateral STEMI.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. Cath lab was activated, and found a 95% proximal LAD occlusion which was stented. It’s unclear if the paramedic ECGs were seen or missed in the ED.
Subtle as a STEMI." (i.e., She was taken to the cath lab, where she was found to have 100% in-stent restenosis of the proximal LAD. In our study, there were 20/53 complete LAD OMI (TIMI-0 flow) which did not meet STEMI criteria. None of the 20 ever evolved to STEMI criteria. This one is easy for the Queen.
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. An open 90% LAD was stented.
I would expect that a stent would be placed. The angiogram showed an open artery with 95% stenosis and thrombosis and it was stented. Quiz : What percent of full blown STEMI have an open artery with normal flow at angiogram? It too is "normal" and you decide that this is not OMI or STEMI and you just decide to get troponins.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? This was stented. Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below).
Many systems now refrain from showing computer "normal" ECGs to the busy emergency physicians at triage because of very poorly conceived articles that say that if the computer algorithm says "normal," the emergency physician should not be bothered. It is clearly missed by the conventional algorithm. Below the limit of detection.
Formula value is now down to a very low value of 19.352 A 90% thrombotic LAD lesion was found and stented. Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4. Finally, Transient STEMI should be taken emergently to the cath lab. The first (and only) ED ECG is here: QTc 386. NTG may cause reperfusion 2.
The near-immediate or instant feedback learning process by which the heart responds to any new invasive procedural variation facilitates each new change; be it drug-eluting stent, drug-coated balloon, or both in different combinations and permutations.
P.S.: Cardiac cath was performed — and showed a distal LA D "culprit" lesion that was successfully stented. It may look identical t o the ST-T wave appearance seen after a STEMI with marked troponin elevation, that has now reperfused ( be this reperfusion spontaneous — or by treatment with PCI or thrombolytics ).
They do not study whether this wave differentiates between MI and non-MI, between STEMI and NonSTEMI, or between OMI and NOMI. Here is an ECG with N-waves, from the article: Are these N-waves in our ECG? Another ECG was recorded: Obvious inferior, posterior, lateral STEMI What is the infarct artery? This is hard to tell.
This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI." He was worried for inferior MI and ordered another, which was recorded 15 minutes later: Now clearly and obviously diagnostic of inferior STEMI. He was found to have a 100% circumflex lesion for which a bare metal stent was placed.
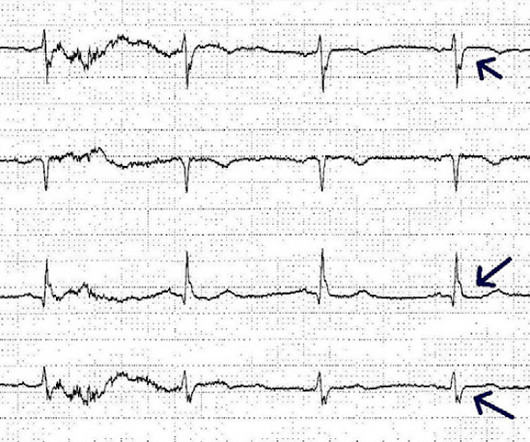
A male in late middle age with a history of RCA stent 8 years prior complained of chest pain. Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiac arrest with unrecognized STEMI, died. EMS recorded the following ECG: What do you see?
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 Here is another classic article. It was stented.
Intra-procedural data included access route, coronary anatomy, lesion complexity, number of stents deployed, door-to-balloon time for primary PCI, and any intra-procedural complications. and the average number of stents 2.6. The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6,
The door to balloon time was incredibly short and there was a 100% circumflex occlusion that was opened and stented. The Non-STEMI, which was an OMI, was diagnosed much faster with AI on the ECG than with troponin. I described "Posterior Reperfusion T-waves" in this article. It had never been described before.
One would not expect wall motion to recover so quickly after stenting, so this is good evidence that the POCUS echo was indeed accurate. Angiogram: Severe diffuse left main disease, up to 80% at the ostial left main. Post cath ECG: Normal or near normal Peak troponin I was 15 ng/mL. Is this OMI?
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
It was opened and stented. Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI. But what we truly care about is coronary occlusion, for which STEMI is just a surrogate that is only about 75% sensitive for occlusion. RCA: dominant.
Here is an article I wrote: Updates on the ECG in ACS. The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present.
See these posts for Wellens' mimics: Pseudo-Wellens' Syndrome due to Left Ventricular Hypertrophy (LVH) Anterior STEMI? It even meets STEMI criteria: 2.5 Is it Wellens' Syndrome? This was the first ECG (ECG #1) recorded during pain : This shows ST elevation and hyperacute T-waves in the LAD distribution.
The patient was then taken to the cath lab an found to have a proximal RCA 100% thrombotic occlusion which was successfully stented. 3) STEMI criteria failed to identify this acute coronary occlusion, like many others. Normal QRS-T angle From this article: Ziegler R and Bloomfield DK.
They were stented. Regional wall motion abnormality-distal septum anterior and apex Today, shortly after this case presented, I received in my inbasket from Journal Feed this article which promotes the idea that "normal" ECGs by computer do not need to be overread by a physician. The peak troponin was 1863 ng/L. Why not very very high?
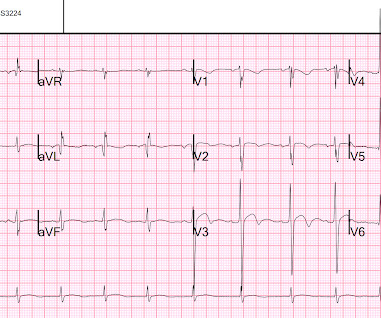
There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI). In fact, the STE is widespread, mimicking an anterior STEMI. Here is full text of this article.
These findings are very subtle but suspicious for LAD occlusion, as we have seen in many similar (but less difficult) cases on this blog: A man in his sixties with chest pain at midnight with undetectable troponin How long would you like to wait for your Occlusion MI to show a STEMI? Learning Points: Not all OMI will present as STEMIs.
Post by Smith, with short article by Angie Lobo ( [link] ), a third year intermal medicine resident at Abbott Northwestern Hospital Case A 30-something woman with no past history, who is very fit and athletic, presented with 1.5 It is equivalent to a transient STEMI. The lesion was stented. hours of substernal chest pressure.
Compare to the anatomy after stenting: The lower of the 2 now easily seen branches is the circumflex, now with excellent flow. As per Dr. Aslanger and his citation of the J Am Heart Assoc article by Meyers, Smith et al — posterior leads are not needed for the diagnosis of acute posterior OMI! The patient recovered well.
Note: according to the STEMI paradigm these ECGs are easy, but in reality they are difficult. Theres inferior STE which meets STEMI criteria, but this is in the context of tall R waves (18mm) and relatively small T waves, and the STD/TWI in aVL is concordant to the negative QRS. This was false positive STEMI with an ECG mimicking OMI.
Case submitted by Andrew Grimes, Advanced Care paramedic, with additions from Jesse McLaren and Smith An 84-year-old male with a notable cardiac history (CABG, multiple stents) woke at 0500hrs with pressure in his chest, diaphoresis, and light-headedness. STEMI criteria are only 43% sensitive for OMI. See our article here.
See our article: Walsh, B., Here is the prehospital ECG, recorded in the presence of pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. A stent was placed. Since this is a young (30 years old!) Macfarlane, P. Prutkin, J.
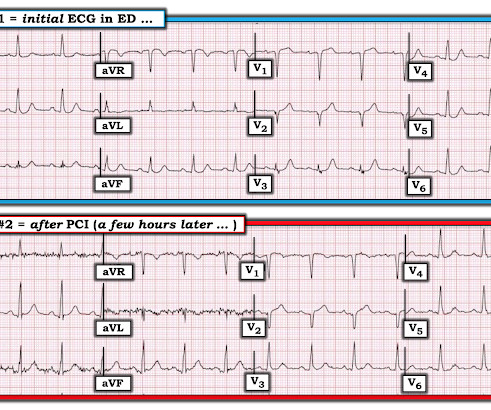
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all.
It is diagnostic of OMI, but this is SUBACUTE OMI I sent this ECG to my "EKG Nerdz" friends, without any clinical info at all and they answered "OMI" The Queen said: "STEMI-Equivalent with High Confidence:" Notice she sees findings in both normal beats and PVCs. It was opened and stented. There are new Q-waves in aVL, V5-6.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content