This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background Hyperglycemia, characterized by elevated blood glucose levels, is frequently observed in patients with acute coronary syndrome, including ST-elevation myocardialinfarction (STEMI). Methods We conducted a comprehensive search for articles on PubMed and Embase using search strategies which yielded 4,061 articles.
She was taken to the cath lab, where she was found to have 100% in-stent restenosis of the proximal LAD. HYPERACUTE T-WAVES ARE EASILY RECOGNIZED BY THE QUEEN OF HEARTS HYPERACUTE T-WAVES DO NOT EVOLVE INTO ST ELEVATION -- THIS IS A MYTH Pendell and I are about to submit an article on ECG findings in total 100% LAD Occlusion (LAD OMI).
So this is indeed diagnostic of myocardialinfarction. Not immediately, at least, because this is NOT diagnostic of ACUTE (occlusion) myocardialinfarction (Acute OMI). So I made an ED diagnosis of Non-Occlusion MyocardialInfarction (NOMI), and his next day angiogram confirmed NOMI.
The near-immediate or instant feedback learning process by which the heart responds to any new invasive procedural variation facilitates each new change; be it drug-eluting stent, drug-coated balloon, or both in different combinations and permutations.
Primary percutaneous coronary intervention (PPCI) remains the gold-standard treatment for ST-elevation myocardialinfarction (STEMI). Additional arterial access via left brachial artery was obtained, and a covered stent was deployed successfully in the right femoral artery with satisfactory haemostasis.
An open 90% LAD was stented. Here is the ECG the next AM: There was so little infarction that there are lateral, but no anterior reperfusion T-waves (normally, there would be Wellens' type waves after LAD reperfusion). Here is some older but very interesting literature on TIMI myocardial perfusion grade and ST resolution : 1.
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronary artery disease and myocardialinfarctions. At that visit the patient was found to have an in-stent RCA occlusion. She's had multiple PCI procedures. Troponin I peaked at 18.323ng/L.
Here is the classic article on continuous 12-lead monitoring (in full text) showing that the ECG is a much more reliable indicator of re-occlusion than are symptoms. Here is another classic article. Consequences of reocclusion after successful reperfusion therapy in acute myocardialinfarction. It was stented.
He was found to have a 100% circumflex lesion for which a bare metal stent was placed. Comment A recently published article (1) found that a computer-interpreted “normal” ECG has a 99% NPV (95% CI: 97-99) for a clinically significant finding. Interventional cardiology was consulted and patient was taken to the cath lab.
Patients in the combination AP +AC therapy group had a higher prevalence of CAD, myocardialinfarction, and coronary/vascular stent placement compared to the AC monotherapy group. The median follow-up of patients was 57 months. The median follow-up of patients was 57 months.
Here is the ED ECG on arrival: Less STE/STD Provider's Clinical Impression: "findings concerning for myocardialinfarction, likely proximal LAD or Left main." One would not expect wall motion to recover so quickly after stenting, so this is good evidence that the POCUS echo was indeed accurate. NTG drip started.
Intra-procedural data included access route, coronary anatomy, lesion complexity, number of stents deployed, door-to-balloon time for primary PCI, and any intra-procedural complications. and the average number of stents 2.6. The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6,
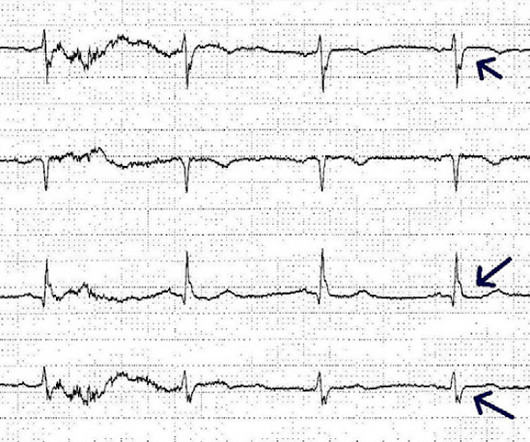
One of our fine interns, Daniel Lee, who is also an ECG whiz, found this paper from 2013 and brought it to my attention: The delayed activation wave in non-ST-elevation myocardialinfarction. Here is an ECG with N-waves, from the article: Are these N-waves in our ECG? The cath lab was activated.
Primary endpoint of systematic review and meta-analysis is the NACE (Net Adverse Cardiac Events) and secondary are MACE (Major Adverse Cardiac Events), mortality, bleedings, myocardialinfarction and stent thrombosis. Subgroup analyses included studies using only ticagrelor-based regimens and three-months duration of DAPT.
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardialinfarction. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J. Am Heart J.
The patient was then taken to the cath lab an found to have a proximal RCA 100% thrombotic occlusion which was successfully stented. Diagnostic and prognostic value of the QRS-T-angle, an ECG marker quantifying heterogeneity of depolarization and repolarization, in patients with suspected non-ST-elevation myocardial infarc tion.
Post by Smith, with short article by Angie Lobo ( [link] ), a third year intermal medicine resident at Abbott Northwestern Hospital Case A 30-something woman with no past history, who is very fit and athletic, presented with 1.5 This is diagnostic of myocardialinfarction. The lesion was stented. Int J Cardiol.
Although not striking, this is clearly a diagnostic ECG for infero"posterior" myocardialinfarction due to coronary occlusion (OMI), most likely due to left circumflex (LCx) artery occlusion. mm STE even in the fourth universal definition of myocardialinfarction. Considerations on the naming of myocardialinfarctions.
They were stented. Regional wall motion abnormality-distal septum anterior and apex Today, shortly after this case presented, I received in my inbasket from Journal Feed this article which promotes the idea that "normal" ECGs by computer do not need to be overread by a physician. The peak troponin was 1863 ng/L. Why not very very high?
Among the patients included, those with diabetes exhibited higher rates of adverse events, including death, spontaneous myocardialinfarction (MI), and repeat revascularization. Original article: Gaba P et al. Pooled data from four trials were analyzed, encompassing patients undergoing PCI or CABG for left main disease.
Background Untreated multivessel disease (MVD) in acute myocardialinfarction (AMI) has been linked to a higher risk of recurrent ischemia and death within one year. Databases were searched for relevant articles published before 10 November 2023.
This was stented. However, this review references the Sterns article above, which by my reading does not state this. I have read articles that say that patients without ischemia are at low risk of complications from hypokalemia, But it is not entirely without risk. After pacing, there was no recurrence of Torsades.
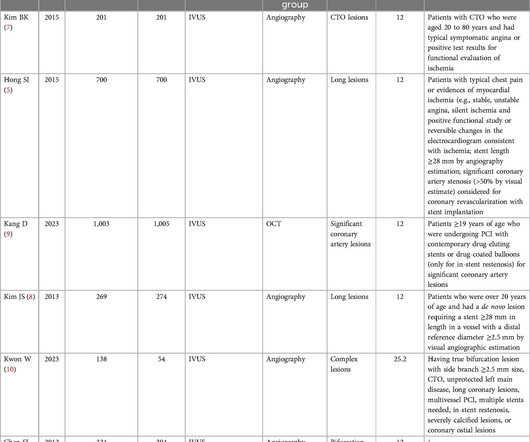
Intravascular imaging (IVI), such as intravascular ultrasound (IVUS) and optical coherence tomography (OCT), play a crucial role in assessing lesion characteristics and optimizing stent placement during percutaneous coronary intervention (PCI). Original article: Kwon W et al. vs 6.7%; HR: 0.77; 95% CI: 0.61-0.97;
In the early years of percutaneous coronary intervention (PCI), studies indicated a heightened risk of major adverse cardiac events (MACE) in patients with reduced left ventricular ejection fraction (LVEF), involving outcomes such as death, Q-wave myocardialinfarction (MI), stent thrombosis, and repeat revascularization.
At the bottom of the post, I have re-printed the section on aVR in my article on the ECG in ACS from the Canadian Journal of Cardiology: New Insights Into the Use of the 12-Lead Electrocardiogram for Diagnosing Acute MyocardialInfarction in the Emergency Department Case 1. Widimsky P et al. J Electrocardiol 2012;45:487-90.
A male in late middle age with a history of RCA stent 8 years prior complained of chest pain. See this article by Widimsky: Primary angioplasty in acute myocardialinfarction with right bundle branch block: should new onset right bundle branch block be added to future guidelines as an indication for reperfusion therapy [link]
Formula value is now down to a very low value of 19.352 A 90% thrombotic LAD lesion was found and stented. The decision to take a patient for emergent reperfusion therapy is largely determined by an ECG diagnostic for ST Elevation MyocardialInfarction (STEMI). The first (and only) ED ECG is here: QTc 386. Hypothesis.
The primary outcome was major adverse cardiac and cerebrovascular event (MACCE), namely a composite of death from cardiovascular causes, myocardialinfarction (MI), stroke, stent thrombosis within 12 month. Patient characteristics and clinical outcomes were collected via electronic medical record system.
This article is part 2 of a series on cardiac CT. If you have not yet read it, I suggest doing so before reading the remainder of this article. I've included the article here. 2 Coronary CT Angiography and 5-Year Risk of MyocardialInfarction. Part one explored the utility and benefits of CT Calcium Scoring.
Here is full text of this article. He was successfully stented. This also confirms right ventricular infarction (RV MI) A follow up TTE demonstrated a normal LVEF with a “regional wall motion abnormality-posterolateral hypokinetic mild, probable.” It was about a 7 minute transport time.
When one of these arteries becomes completely blocked by a blood clot, it results in a heart attack, also known as MI (Myocardialinfarction). When a person experiences a heart attack or myocardialinfarction, they may feel chest pain and other symptoms in different parts of their body.
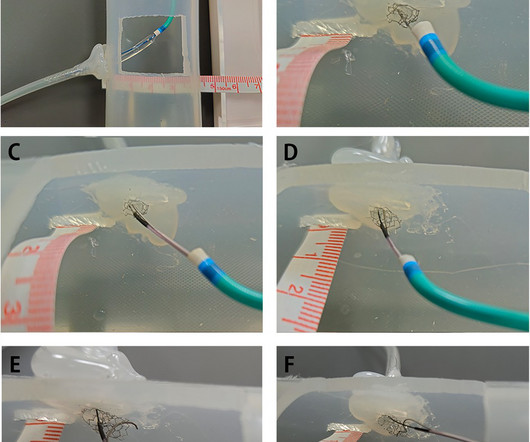
BackgroundPercutaneous coronary intervention (PCI) through the aorto-ostial coronary stent that is protruding into the aorta remains a technical challenge because of the poor coaxial alignment of the guiding catheter and the inability to advance the guidewire into the distal vessel through the stent's central lumen.
Case submitted by Andrew Grimes, Advanced Care paramedic, with additions from Jesse McLaren and Smith An 84-year-old male with a notable cardiac history (CABG, multiple stents) woke at 0500hrs with pressure in his chest, diaphoresis, and light-headedness. See our article here. He had a 100% RCA occlusion which was stented.
It was opened and stented. Compared to TTE from 7/3/24: the anterior regional wall motion abnormality is new and is consistent with ischemia/infarction in the LAD territory == MY Comment , by K EN G RAUER, MD ( 11/20 /2024 ): == There are several insightful aspects of today's case. This is then a large MI, but it is subacute.
We included major adverse cardiovascular events (MACE), myocardialinfarction (MI), cardiac death and other outcome indicators. ConclusionsCompared with the non-IVUS-guided group, IVUS-guided stent implantation may be more effective for patients with complex CAD.Systematic Review RegistrationPROSPERO [CRD42024531366].
See our article: Walsh, B., A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. A stent was placed.
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content