This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
One of the most common questions I get is, “ Do I need a stent to treat my heart disease?” ” Typically, several of this person’s friends have had stents, so it seems natural to ask. First, we must understand what a stent is and why it is used. The stent ‘unblocks’ it. Flow is restored.
ECG#1 Assessing ischemia on an ECG with wide QRS complexes (AIVR, ventricular pacing, BBB, etc) can be challenging. Many health care providers will simply not attempt to assess ischemia in the presence of a wide QRS. In the ECG above there are several features indicative of ongoing transmural ischemia. What do you think?
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. The ECG only tells you there is ischemia, not the etiology of it. Nevertheless, the clinical situation made other etiologies unlikely.
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? The last echocardiography 12 months ago showed HFmrEF.
Background Untreated multivessel disease (MVD) in acute myocardial infarction (AMI) has been linked to a higher risk of recurrent ischemia and death within one year. Databases were searched for relevant articles published before 10 November 2023. Pertinent data from the included studies were extracted and analyzed using RevMan v5.4.
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? Here is an article I wrote: Updates on the ECG in ACS. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present.
I would expect TIMI-3 flow (normal flow, no persistent ischemia) with a culprit in the RCA (or possibly Circumflex). I would expect that a stent would be placed. The angiogram showed an open artery with 95% stenosis and thrombosis and it was stented. What would I expect the angiogram to show? Jesse McLaren et al.
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." Here is another classic article. It was stented. Eur Heart J 2001;22:1997–2006. Gottlieb SO, et al.
But it was interpreted as no acute ischemia and the patient was referred to cardiology as Non-STEMI. The total occlusion was recanalized and stented from 100 to 0%. Clinical: patient alerts for refractory ischemia (refractory chest pain), and empowering nurses to advocate for patients 4. Hyperacute T-waves remain in V3 and V4.
Down-up T-waves in inferior leads are almost always reciprocal to ischemia in the territory underlying aVL. This is not normal and is a tip off that there is posterior ischemia accompanying the ischemia in aVL. It was opened and stented. Data from stress testing proves that the ST depression of ischemia does not localize.
Below is the first ECG recorded by paramedics after 2 hours of chest pain, interpreted by the machine as “possible inferior ischemia”. Cath lab was activated, and found a 95% proximal LAD occlusion which was stented. What do you think? But the care of this and other patients could have been improved with earlier detection of OMI.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
This article is part 2 of a series on cardiac CT. If you have not yet read it, I suggest doing so before reading the remainder of this article. I've included the article here. 5 ISCHEMIA Research Group. Part one explored the utility and benefits of CT Calcium Scoring. Eur Heart J. 2020 Jan 14;41(3):407-477. N Engl J Med.
The patient was then taken to the cath lab an found to have a proximal RCA 100% thrombotic occlusion which was successfully stented. Normal QRS-T angle From this article: Ziegler R and Bloomfield DK. Yes, there are valuable articles from 50 years ago! Progression of V2 showing posterior involvement.
Post by Smith, with short article by Angie Lobo ( [link] ), a third year intermal medicine resident at Abbott Northwestern Hospital Case A 30-something woman with no past history, who is very fit and athletic, presented with 1.5 The lesion was stented. It they are static, then they are not due to ischemia.
This transmural ischemia, but not necessarily completed infarction (yet). See more images of this case at Gopal's Spectral CT Blog: It's all about confidence With continued symptoms, an elevated troponin, and no other explanation, this is acute MI with ongoing ischemia until proven otherwise.
An open 90% LAD was stented. A 51 year old male with h/o stent presented with 30 minutes of chest pain: Obvious anterolateral very acute STEMI with hyperacute T-waves He went for immediate PCI, with successful reperfusion of a 100% occluded proximal LAD, and a door to balloon time of 35 minutes. The LAD has reperfused early.
This was stented. If there is polymorphic VT with a long QT on the baseline ECG, then generally we call that Torsades, but Non-Torsades Polymorphic VT can result from ischemia alone. However, this review references the Sterns article above, which by my reading does not state this. The patient stabilized. Crit Care Med.
Compare to the anatomy after stenting: The lower of the 2 now easily seen branches is the circumflex, now with excellent flow. Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia). The patient recovered well. J Am Heart Assoc.
100% proximal LAD thrombotic occlusion with TIMI 0 flow was found and stented with excellent angiographic result and TIMI 3 flow. When in doubt, record serial ECGs and watch out for signs of ischemia despite medical management. == Comment by K EN G RAUER, MD ( 7/11/2019 ): == Our thanks to Drs. Cath images: Before intervention.
RCA ischemia often results in sinus bradycardia from vagal reflex or ischemia of the sinus node. Here is full text of this article. He was successfully stented. A narrow complex bradycardia without any P-waves is also likely to respond to atropine, as it may be a junctional rhythm.
Case submitted by Andrew Grimes, Advanced Care paramedic, with additions from Jesse McLaren and Smith An 84-year-old male with a notable cardiac history (CABG, multiple stents) woke at 0500hrs with pressure in his chest, diaphoresis, and light-headedness. See our article here. He had a 100% RCA occlusion which was stented.
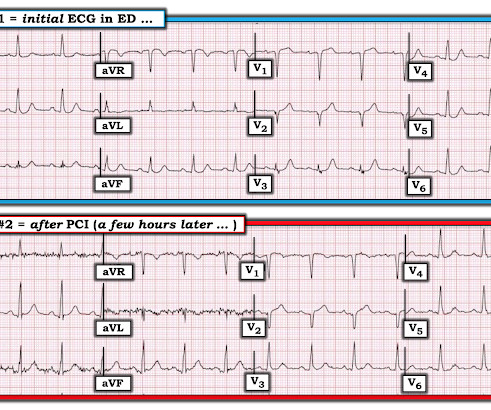
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all.
It was opened and stented. Compared to TTE from 7/3/24: the anterior regional wall motion abnormality is new and is consistent with ischemia/infarction in the LAD territory == MY Comment , by K EN G RAUER, MD ( 11/20 /2024 ): == There are several insightful aspects of today's case. The November 10, 2020 post — for PTA.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content