This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
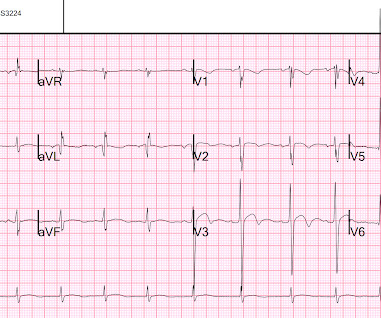
Written by Jesse McLaren A healthy 75 year old developed 7/10 chestpain associated with diaphoresis and nausea, which began on exertion but persisted. Below is the first ECG recorded by paramedics after 2 hours of chestpain, interpreted by the machine as “possible inferior ischemia”. What do you think?
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis.
A male in late middle age with a history of RCA stent 8 years prior complained of chestpain. EMS recorded the following ECG: What do you see? The computer read "Right Bundle Branch Block" There is RBBB and LAFB, which can make it difficult to see the end of the QRS.
An elderly woman presented with chestpain that radiated to the back for several hours. The first troponin returned at 0.099 ng/mL (elevated, consistent with Non-Occlusion MI) Providers were concerned with aortic dissection, so they order a chest aorta CT. Here is here initial ECG: There is only a nonspecific flat T-wave in aVL.
Written and submitted by Ashley Mogul, with edits by Pendell Meyers and Steve Smith A man in his 40s with recent smoking cessation but otherwise no known past medical history presented due to chestpain since the previous evening. The pain has been constant and associated with vomiting and diaphoresis.
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. Case A 40-something male presented to triage. There are classic Wellens' waves in V2-V5.
One of the most common questions I get is, “ Do I need a stent to treat my heart disease?” ” Typically, several of this person’s friends have had stents, so it seems natural to ask. First, we must understand what a stent is and why it is used. The stent ‘unblocks’ it. Flow is restored.
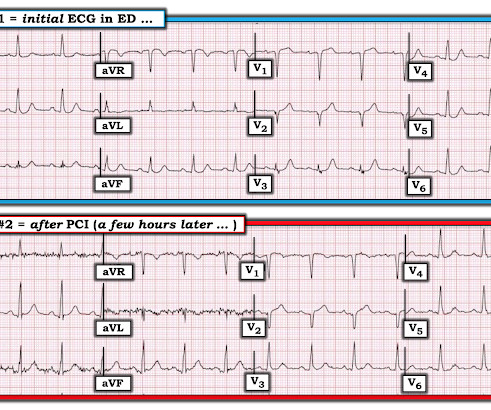
A 60-something awoke with 10/10 crushing chestpain. I would expect that a stent would be placed. The angiogram showed an open artery with 95% stenosis and thrombosis and it was stented. But the patient's chestpain continues and so you order a 2nd ECG (ECG 2 here). He walked in to triage.
P.S.: Cardiac cath was performed — and showed a distal LA D "culprit" lesion that was successfully stented. The following are the KEY clinical and ECG features that establish the diagnosis of W ellens ' S yndrome : There should be a history of prior chestpain that has resolved at the time the defining ECG is obtained.
After only 90 minutes of chestpain, the first troponin was unsurprisingly in the normal range at 11ng/L (normal <26 in males and <16 in females), so the emergency physician waited for repeat troponin. Chestpain still persists. Paged cardiology 0800: patient complains of chestpain. Cardiology aware.
Sent by anonymous A man in his 40s with no previous heart disease presented within 30 minutes of onset of acute chestpain that started while exercising. Successful drug-eluting stent placement opening up 95% mid RCA stenosis to 0% residual Nonobstructive left system disease. Chestpain and a computer ‘normal’ ECG.
The patient's chestpain had resolved by the time of the ECG 2. But it does prove that the patient has coronary disease and makes the probability that his chestpain is due to ACS very very high. Angiogram: Widely patent RCA and LAD stents. Therefore, no stent was placed. (No There are well-formed Q-waves 3.
On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. At that visit the patient was found to have an in-stent RCA occlusion. The patient was referred emergently to the cath lab, and again there was an in-stent RCA occlusion. What do you think? Troponin I peaked at 18.323ng/L.
This patient had the onset of chestpain 24 hours before arrival to the ED. The door to balloon time was incredibly short and there was a 100% circumflex occlusion that was opened and stented. I described "Posterior Reperfusion T-waves" in this article. Here is that ECG: Original ECG What do you think?
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chestpain. EMS gave 324 mg aspirin and 3 sublingual NTG, which the patient stated reduced the substernal chestpain from an 8/10 to 4/10. The ECG only tells you there is ischemia, not the etiology of it.
This article is part 2 of a series on cardiac CT. If you have not yet read it, I suggest doing so before reading the remainder of this article. I've included the article here. Regardless, if you present with chestpain and get a stress test instead of a CTCA, you are arguably getting an inferior test.
This 42 yo diabetic male presented with cough and foot pain. In spite of aggressive questioning, he denied chestpain, but he did tell one triage nurse that he had had some chest burning, and so he underwent an ECG: There are deep Q-waves and QS-waves in precordial leads V2-V3, with a bit of R-wave left in V4.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. It was stented.
This was sent by : Jacob Smith, DO Emergency Medicine Resident Ohio Health Doctors Hospital Emergency Residency Christopher Lloyd, DO, FACEP Director of Clinical Education, USACS Midwest Case A 30 year old patient presents to triage with chestpain. link] Here is the history: A 30 yo man presented complaining of severe chestpain.
She went on to describe her chestpain as a "buffalo sitting on my chest" and a "weird" sensation in her jaw for 1 hour prior to arrival, associated with lightheadedness and diaphoresis. The patient was given fentanyl initially for chestpain with minimal effect and then vomited which was followed by zofran and famotidine.
This 50-something otherwise healthy male presented with one hour of epigastric and lower chestpain. Here is an ECG with N-waves, from the article: Are these N-waves in our ECG? A 100% occlusion on of the circumflex, proximal to the first obtuse marginal, was found, opened, and stented. The cath lab was activated.
Post by Smith, with short article by Angie Lobo ( [link] ), a third year intermal medicine resident at Abbott Northwestern Hospital Case A 30-something woman with no past history, who is very fit and athletic, presented with 1.5 hours of substernal chest pressure. The lesion was stented. She had zero CAD risk factors.
A middle-aged male called 911 for chestpain. Here was the first prehospital ECG with pain at 5/10: Computerized QTc is 418 ms. Formula value is now down to a very low value of 19.352 A 90% thrombotic LAD lesion was found and stented. There is nondiagnostic ST elevation in V1-V4. Most ST elevation is resolved.
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. She presented to the emergency department after a couple of days of chest discomfort. Many advances in treatment have occurred in the 28 years since this article was published. The last echocardiography 12 months ago showed HFmrEF.
Case A 47 year old male called 911 for severe chestpain. It was opened and stented. A woman in her 60s with no prior history of CAD presented with 3 hours of sharp, centrally located chestpain with radiation to the anterior neck, with associated nausea. Culprit, stented) 3. He was clammy and looked unwell.
A 40 something otherwise healthy man presented with substernal chestpain. They were stented. As noted by Dr. Smith — the Am J Emerg Med article he cites above floats the notion that ECGs interpreted as "normal" by the computer "do not need to be overread by a physician". What do you think? Why not very very high?
Case A 39-year-old male without prior medical history presents with chestpain that started 2 hours prior to presentation. He says that the pain intensity was 10/10 at home but now about 4/10. Despite the clinical stability and decreasing pain, this patient needs an immediate angiogram. Here are his publications.)
At the bottom of the post, I have re-printed the section on aVR in my article on the ECG in ACS from the Canadian Journal of Cardiology: New Insights Into the Use of the 12-Lead Electrocardiogram for Diagnosing Acute Myocardial Infarction in the Emergency Department Case 1. This is her ECG: An obvious STEMI, but which artery?
A late middle-aged man presented with one hour of chestpain. This was stented. However, this review references the Sterns article above, which by my reading does not state this. Most recent echo showed EF of 60%. He also had a history of chronic kidney disease, stage III. He had recently had a NonSTEMI. Crit Care Med.
Patient 2 : 55 year old with 5 hours of chestpain radiating to the shoulder, with nausea and shortness of breath ECG: sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. This was missed by the treating physician, but the chestpain resolved with aspirin. This was STEMI(-)OMI.
When a person experiences a heart attack or myocardial infarction, they may feel chestpain and other symptoms in different parts of their body. This article delves into heart attack symptoms, golden hour, treatment & prevention. The sooner you identify the symptoms, the quicker you can take action.
Case submitted by Andrew Grimes, Advanced Care paramedic, with additions from Jesse McLaren and Smith An 84-year-old male with a notable cardiac history (CABG, multiple stents) woke at 0500hrs with pressure in his chest, diaphoresis, and light-headedness. The patient has acute persistent refrectory chestpain and elevated troponin.
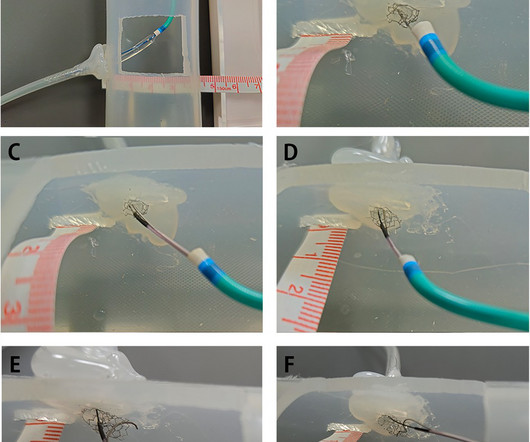
BackgroundPercutaneous coronary intervention (PCI) through the aorto-ostial coronary stent that is protruding into the aorta remains a technical challenge because of the poor coaxial alignment of the guiding catheter and the inability to advance the guidewire into the distal vessel through the stent's central lumen.
A 30 year old African American Male presented to the ED with chestpain that occurred the day before. There was no pain on the day of presentation. See our article: Walsh, B., What do you think the prehospital ECG showed (with pain)? This male in his 40's had been having intermittent chestpain for one week.
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all.
1) Very high initial troponin of 45,000 ng/L 2) A full day of chestpain 3) Q-waves on the ECG, with some T-wave inversion Here is one frame of the CT scan which includes the heart: Can you spot the infarct? It was opened and stented. SUBACUTE) OMI, that would result in an undesirable delay. How do I know?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content