This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A small proportion of patients with STEMI treated via primary PCI experienced late ventricular tachycardia (VT) or ventricular fibrillation (VF), occurring one or more days following the procedure, but late VT or VF with cardiacarrest occurred rarely, especially among patients with uncomplicated STEMI, according to a study published in JAMA Network (..)
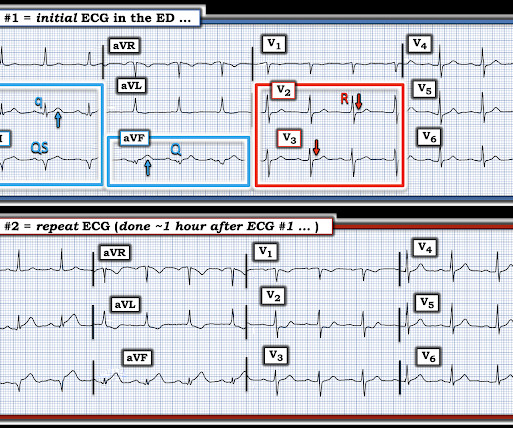
Subtle as a STEMI." (i.e., About 45 minutes after the second EKG, the patient was found in cardiacarrest. Later the next day, she went into cardiacarrest again. By the time I saw the repeat EKG, the patient was already in cardiacarrest. None of the 20 ever evolved to STEMI criteria.
Here is an article I wrote: Updates on the ECG in ACS. The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present.
Primary percutaneous coronary intervention (PPCI) remains the gold-standard treatment for ST-elevation myocardial infarction (STEMI). We present the case of a man in his 50s, admitted with cardiacarrest secondary to inferolateral STEMI.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. The patient had ROSC and maintained it.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? I was texted these ECGs by a recent residency graduate after they had all been recorded, along with the following clinical information: A 50-something with no cardiac history, but with h/o Diabetes, was doing physical work when he collapsed.
Discussion See this post: STEMI with Life-Threatening Hypokalemia and Incessant Torsades de Pointes I could find very little literature on the treatment of severe life-threatening hypokalemia. If cardiacarrest from hypokalemia is imminent (i.e., When the ECG shows the effects of hypokalemia, it is particularly dangerous.
This is a troponin I level that is almost exclusively seen in STEMI. I suspect this is Type 2 MI due to prolonged severe hypotension from cardiacarrest. So this is either a case of MINOCA, or a case of Type II STEMI. If the arrest was caused by acute MI due to plaque rupture, then the diagnosis is MINOCA.
Could this be Septal STEMI (STE in V1 and aVR, with reciprocal ST depression in V4-V6?), Aslanger added in the limitations in his article: " Theoretically, an isolated basal inferoseptal infarction or an acute inferior MI in the presence of previous infarctions that may change the orientation of lesion vector can also cause a similar picture.
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. In a recent article (J Electrocardiol this year, see reference below), peak trop onin I levels in takotsubo presenting with ST Elevation were median 1.02 She was defibrillated and resuscitated. ng/mL [IQR: 0.46, 2.35].
If cardiacarrest from hypokalemia is imminent (i.e., However, this review references the Sterns article above, which by my reading does not state this. to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 Give an initial infusion of 10 mEq IV over 5 minutes; repeat once if needed. *The
He had a previous MI with cardiacarrest 2 years prior. Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI. The ST depression may be the most visibly obvious sign of STEMI. Some are STEMI-equivalents.
A prehospital ECG was recorded (not shown and not seen by me) which was worrisome for STEMI. A previous ECG from 4 years prior was normal: This looks like an anterior STEMI, but it is complicated by tachycardia (which can greatly elevate ST segments) and by the presentation which is of fever and sepsis.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
4 Unfortunately, this article provides no electrocardiographic, echo, or angiographic data, so it is not certain that these high levels were in the absence of acute MI. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease.
Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiacarrest with unrecognized STEMI, died. Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAH) on the admission ECG.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. baseline (this is what most recommend but seems like far too much QRS widening to me) = See these articles and this graphic: 1. The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chest pain.
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". Hyperkalemia mimics STEMI and OMI in many distributions, but probably the most common is the Brugada morphology in V1-V2 which mimics anterior OMI for those who cannot recognize the Brugada pattern. HyperKalemia with CardiacArrest.
The article is edited by Smith. 2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. This was submitted by Alexandra Schick. Bicarb 20, Lactate 4.2, Ammonia 100.
Here is the PMcardio Queen of Hearts interpretation of the ECG: STEMI equivalent detected. Inferior and posterior OMI without STEMI criteria. About an hour later another ECG was obtained: Barely meets STEMI criteria in inferior leads, but obvious inferior and posterior OMI. The cath lab was now activated for STEMI.
Further history later: This patient personally has no further high risk features (syncope / presyncope), but her mother had sudden cardiacarrest in sleep. We repeated the ECG: Brugada pattern is mostly resolved. Follow up the next AM: Brugada pattern is resolved Below is what the electrophysiologist recommended.
The paramedics diagnosis was "Possible Anterolateral STEMI." More proof that a huge STEMI may have normal or near normal initial troponin. We showed this in this article in JAMA Cardiology. A retrospective 'target trial emulation' comparing amiodarone and lidocaine for adult out-of-hospital cardiacarrest resuscitation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content