This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
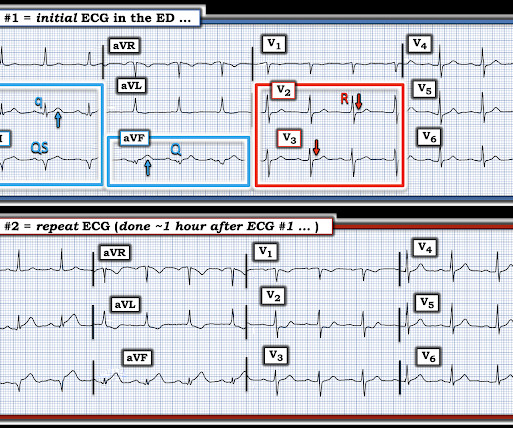
About 45 minutes after the second EKG, the patient was found in cardiacarrest. Later the next day, she went into cardiacarrest again. By the time I saw the repeat EKG, the patient was already in cardiacarrest. Hyperacute T Wave in the Early Diagnosis of Acute MyocardialInfarction.
Impella and venoarterial extracorporeal membrane oxygenation (VA-ECMO) in patients with acute myocardialinfarction-related cardiogenic shock (AMICS). Impella patients were older (34% vs. 13% >75 years, p < 0.001) and less frequently presented after an out-of-hospital cardiacarrest (18% vs. 40%, p < 0.001).
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. The patient had ROSC and maintained it.
Primary percutaneous coronary intervention (PPCI) remains the gold-standard treatment for ST-elevation myocardialinfarction (STEMI). We present the case of a man in his 50s, admitted with cardiacarrest secondary to inferolateral STEMI.
In this case, profound shock for 1 hour would result in the same degree of infarction. I suspect this is Type 2 MI due to prolonged severe hypotension from cardiacarrest. A followup ECG was recorded 2 days later: No definite evidence of infarction. This is a troponin I level that is almost exclusively seen in STEMI.
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. In a recent article (J Electrocardiol this year, see reference below), peak trop onin I levels in takotsubo presenting with ST Elevation were median 1.02 She was defibrillated and resuscitated. ng/mL [IQR: 0.46, 2.35].
Both of these patterns together suggest Aslanger's pattern , recently published in J Electrocardiology: A new electrocardiographic pattern indicating inferior myocardialinfarction. These suggest inferior OMI with possible RV involvement. Could this be Septal STEMI (STE in V1 and aVR, with reciprocal ST depression in V4-V6?),
The study utilized the ISCHEMIA primary outcome, a composite measure of cardiovascular death, protocol-defined myocardialinfarction, or hospitalization for unstable angina, heart failure, or resuscitated cardiacarrest. Original article: Redfors B et al. years, with 57.1% occurring within 30 days after CABG.
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. For this reason, some argue that it should not be measured in patients unless acute myocardialinfarction is on the differential diagnosis.
If cardiacarrest from hypokalemia is imminent (i.e., However, this review references the Sterns article above, which by my reading does not state this. As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 mEq/L for every 100 mEq total body deficit. mEq/L, from 1.9
The short answer is ‘ Yes ’ But if you want to know why and what you can do about it, you should read the rest of this article. And pretty much every doctor can recall an event where a patient experienced a suddenly stressful event and had a cardiac event. Does stress cause heart disease? to the adversity you face in life.
Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiacarrest with unrecognized STEMI, died. Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAH) on the admission ECG.
The cause of CS was acute myocardialinfarction in 438 (63.9%) patients, and 431 (62.9%) patients presented with cardiacarrest. interquartile range 4.112.7] A total of 410 patients (59.9%) were successfully weaned from VA-ECMO, whereas in 275 patients (40.1%) weaning failed (i.e.
Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). baseline (this is what most recommend but seems like far too much QRS widening to me) = See these articles and this graphic: 1. Inotropic medication was continued.
Original article: Gaudino M et al. However, it remains unclear whether these lower referral rates for women stem from physician bias, disparities in baseline clinical status, or differences in the extent of coronary artery disease. EuroIntervention. 2024 Mar 5:EIJ-D-24-00011.
You can read the abstract (o r of course the entire article) at the link provided. Pharmacological facilitation of primary percutaneous coronary intervention for acute myocardialinfarction: is the slope of the curve the shape of the future? (And, Inferior and posterior OMI without STEMI criteria. Very interesting.
We showed this in this article in JAMA Cardiology. REFERENCE Prevention of primary ventricular fibrillation in acute myocardialinfarction with prophylactic lidocaine [link] Primary ventricular fibrillation (VF) during an acute myocardialinfarction (AMI) occurs with a high incidence and mortality rate with or without thrombolysis.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content