This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. The patient had ROSC and maintained it.
A small proportion of patients with STEMI treated via primary PCI experienced late ventricular tachycardia (VT) or ventricular fibrillation (VF), occurring one or more days following the procedure, but late VT or VF with cardiacarrest occurred rarely, especially among patients with uncomplicated STEMI, according to a study published in JAMA Network (..)
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
Case A 47 year old male called 911 for severe chestpain. He had a previous MI with cardiacarrest 2 years prior. A woman in her 60s with no prior history of CAD presented with 3 hours of sharp, centrally located chestpain with radiation to the anterior neck, with associated nausea.
Aslanger added in the limitations in his article: " Theoretically, an isolated basal inferoseptal infarction or an acute inferior MI in the presence of previous infarctions that may change the orientation of lesion vector can also cause a similar picture. Could this be Septal STEMI (STE in V1 and aVR, with reciprocal ST depression in V4-V6?),
If a patient presents with chestpain and a normal heart rate, or with shockable cardiacarrest, then ischemic appearing ST elevation is STEMI until proven otherwise. It is important to remember that not every acute MI with ST elevation is the result of acute coronary occlusio n. Clinical Context is everything !
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
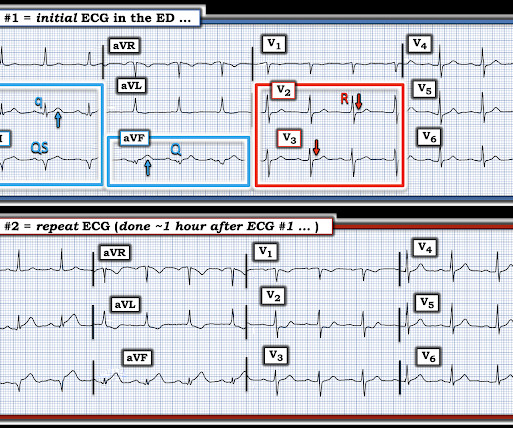
And the article was rejected. LEARNING Point: Maximal ST depression in leads V2-thru-V4 ( especially when the ST-T waves are shaped as they are in ECG #1 ) in a patient with new chestpain ( or sudden cardiacarrest, as in today’s case ) — is diagnostic of acute Posterior OMI until proven otherwise!
A male in late middle age with a history of RCA stent 8 years prior complained of chestpain. Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiacarrest with unrecognized STEMI, died. EMS recorded the following ECG: What do you see?
A late middle-aged man presented with one hour of chestpain. If cardiacarrest from hypokalemia is imminent (i.e., However, this review references the Sterns article above, which by my reading does not state this. As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Written By Magnus Nossen — with edits by Ken Grauer and Smith. The below ECG was recorded.
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. Steve, what do you think of this ECG in this CardiacArrest Patient?" What is it?
This article discusses correction of the QT interval for rate. The article is written by Dr. Smith and Dr. Friedman. The last sections of this article are on the QT interval and is essential reading : Here are some pearls from this article before we get started : 1. now an EM resident at Beth Israel.
The article is edited by Smith. It was from a patient with chestpain: Note the obvious Brugada pattern. This was submitted by Alexandra Schick. Dr. Schick is a PGY3 at the Brown Emergency Medicine Residency in Rhode Island. I remember Allie well from her days in the Research volunteer program at Hennepin.
Further history later: This patient personally has no further high risk features (syncope / presyncope), but her mother had sudden cardiacarrest in sleep. The patient denied any chestpain whatsoever, and a troponin at zero and 2 hours were both undetectable. We repeated the ECG: Brugada pattern is mostly resolved.
Written by Pendell Meyers, sent by anonymous, with additions by Smith A man in his 40s had acute chestpain and called EMS. You can read the abstract (o r of course the entire article) at the link provided. We are lucky this patient did not have a cardiacarrest while in the Waiting Room. Very interesting.
A middle-age woman with no previous cardiac history called 911 for chestpain. We showed this in this article in JAMA Cardiology. A retrospective 'target trial emulation' comparing amiodarone and lidocaine for adult out-of-hospital cardiacarrest resuscitation. The final angiographic result is very good.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content