This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
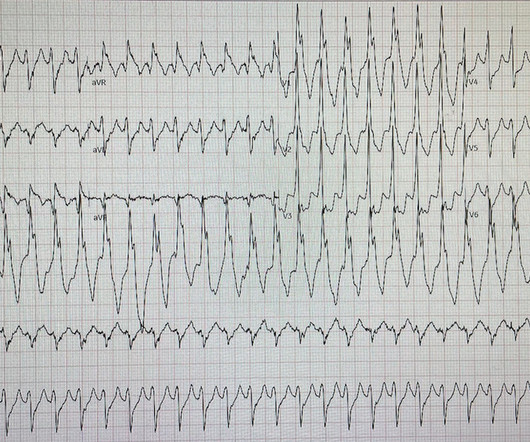
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
NOTE: The ECG in Figure-1 has been recorded at the usual 25mm/second speed — but with the Cabrera format ( Please see my Editorial Note near the top of the page in ECG Blog #365 for review of the basics of this recording system ). ECG Blog #185 — Review of the P s, Q s, 3 R Approach for systematic rhythm interpretation.
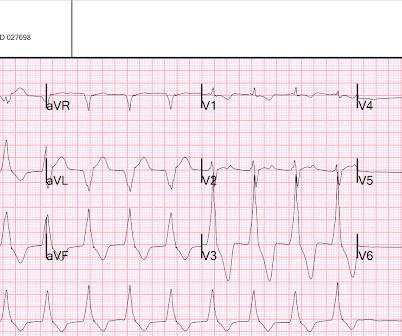
Readers of the Smith ECG Blog will probably recognize this a very subtle inferior OMI. The VT vs SVT with Aberrancy debate is beyond the scope of this particular blog post. Helpful tools to differentiate a WCT ECG include the Smith ECG Blog, and the Life in The Fast Lane blog. Here is the ECG after 200J.
She was awake, alert, well perfused, with normal mental status and overall unremarkable physical exam except for a regular tachycardia, possible rales at both bases, some mild RUQ abdominal tenderness. Thus, I believe it is a regular, monomorphic, wide complex tachycardia. Or it could simply still be classic VT. What is the Diagnosis?
There were times when it would be usurped by sinus tachycardia, then return to this rhythm. I had a previous case of an adolescent with trauma and chest pain who also had AIVR: An adolescent with trauma, chest pain, and a wide complex rhythm From this blog post: "AIVR is NOT common in otherwise healthy children. It is irregular.
A young male with unknown past medical history presents with AMS and tachycardia. There is sinus tachycardia, a prolonged QRS (computer read it as 114 ms, previous ECG with 102 ms). But because the physicians were so focused on his tachycardia, meth use, and rhythm, they did not look for or appreciate the findings of TCA overdose.
NOTE: The ECGs in today's case are recorded in the Cabrera Format ( See Dr. Grauer Comment in the October 26, 2020 post of Dr. Smith's ECG Blog for review on the Cabrera Format ). The 2019 ESC Guidelines for the management of patients with supraventricular tachycardia indicated that IV Amiodarone should not be considered in these populations.
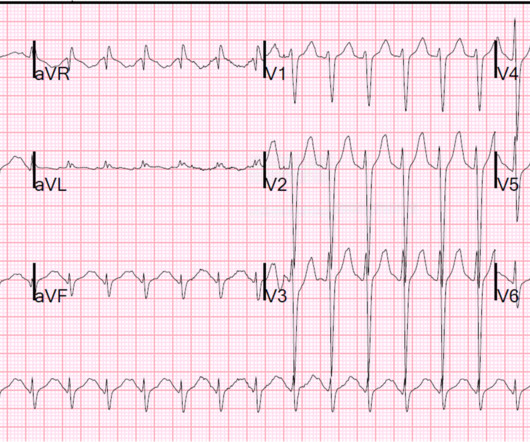
They had already cardioverted at 120 J, then 200 J, which resulted in the following: Ventricular Tachycardia They then cardioverted at 200 J which r esulted in the same narrow complex rhythm shown above, at 185 beats per minute. This would treat both SVT or sinus tachycardia. I suggested esmolol if the heart rate did not improve.
The team immediately paged cardiology, concerned for polymorphic ventricular tachycardia. Since sinus conducted QRS complexes cannot co-exist together with ventricular tachycardia, this must all be artifact. The rhythm terminated before it could be captured on 12-lead. Upon questioning, the patient reported palpitations.
This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). baseline (this is what most recommend but seems like far too much QRS widening to me) = See these articles and this graphic: 1.
Multifocal Atrial Tachycardia 2. Full text online: [link] Here are excerpts from the article: From the Introduction: Among rhythm diagnoses, atrial fibrillation (AF) is particularly important for appropriate management. The rhythm is indeed irregularly irregular, so atrial fibrillation must be considered. Sinus with multifocal PACs 3.
and tachycardia, 1.8. Finally , they found that S1Q3T3, precordial T-wave inversions V1-V4, and tachycardia were independent predictors of PE. In the Marchik article, (assuming they defined it the same way, and the methods do not specify this), S1Q3T3 was found in 8.5% They found that S1Q3T3 had a Positive Likelihood Ratio of 3.7,
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. I said I think there is a fixed stenosis in the LAD and the tachycardia and stress caused a type 2 STEMI.
This is sinus tachycardia (rhythm) with complete heart block (AV node function) with ventricular escape rate just below 30. Never forget that sinus tachycardia is the scariest arrhythmia. The September 27, 2019 post — for the Rowlands & Moore article with the above-noted formulas for recognizing the “culprit” extremity.
We can see enough to make out that the rhythm is sinus tachycardia. Tachycardia is unusual for OMI, unless the patient is in cardiogenic shock (or getting close). A bedside ultrasound should be done to assess volume and other etiologies of tachycardia, but if no cause of type 2 MI is found, the cath lab should be activated NOW.
This one is far more specific, as it is combined with sinus tachycardia and some T-wave inversion in V1-V3. and tachycardia, 1.8. Finally , they found that S1Q3T3, precordial T-wave inversions V1-V4, and tachycardia were independent predictors of PE. This is a classic S1Q3T3. Most S1Q3T3 is not due to PE. incomplete RBBB 1.7
This ECG has Q-waves, but they are not very wide nor very deep, and so I doubt that the inferior STE is due to old MI. See these posts: Chest Pain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab?
Here is his 12-lead ECG: The computer reads supraventricular tachycardia. In these cases, they were misdiagnosed as sinus tachycardia (not PSVT): Notice there is a "P-wave" just before the QRS in V1 Notice there is a "P-wave" directly superimposed (on top of) the T-wave in V1. Narrow complex tachycardia at rate of 135.
Tachycardia (or nearly) 2. In the Marchik article, (assuming they defined it the same way, and the methods do not specify this), among patients with suspicion for PE, S1Q3T3 was found in 8.5% Tachycardia, = 1.8. Finally , they found these independent predictors of PE: Note that tachycardia only has an Odds ratio of 1.8.
The findings include sinus tachycardia, characteristic QRS morphology most diagnostic in V3 with a small R wave followed by a very large S wave with a convex upward ST segment morphology, ST segment strain morphology in the inferior and anterior leads leading to deep symmetric T-wave inversion. and tachycardia, 1.8. incomplete RBBB 1.7
This article discusses correction of the QT interval for rate. I've been working on this a long time, thought about submitting it to a journal, but decided it gets more readers on this blog. The article is written by Dr. Smith and Dr. Friedman. In that article, they do not say what is a dangerously short QT is (e.g.
A rapid heartbeat (tachycardia) can increase the workload on your heart, while a slow heartbeat (bradycardia) can cause fatigue and dizziness. Related Article: Medications for Congenital Heart Disease: What Every Parent Should Know Give Hope 365 Days a Year.
While this blog post has been reviewed by clinical experts, it does not substitute for personalized advice from your healthcare providers. Antiarrhythmic Drugs WHAT THEY DO : Antiarrhythmic drugs are used to help prevent or treat abnormal heart rhythms, such as atrial fibrillation and ventricular tachycardia.
The article is edited by Smith. Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. This was submitted by Alexandra Schick. Dr. Schick is a PGY3 at the Brown Emergency Medicine Residency in Rhode Island.
T-wave inversions and dynamic ST elevation Tachycardia, hyperthyroid, and ST elevation. Please see My Comment at the bottom of the page in the April 17, 2022 post of Dr. Smith's Blog — for concise review on how to quickly recognize too-high placement of the lead V1 and V2 electrodes. He was discharged. What is it? Anterior STEMI?
And the article was rejected. This blog is full of cases in which OMI that did not meet STEMI millimeter criteria were dismissed. MY Thoughts on ECG #1: The rhythm is sinus tachycardia at 105-110/minute. The 4th universal definition mentions ST depression, posterior MI, and T-wave changes." The PR and QRS intervals are normal.
After initiating treatment for hyperkalemia, repeat ECG showed resolution of Brugada pattern: The ECG shows sinus tachycardia. A Very Wide Complex Tachycardia. Regarding BRUGADA Syndrome vs Phenocopy: We’ve presented many cases of Brugada ECG patterns on Dr. Smith’s ECG Blog. The QRS is narrow and T waves are much less peaked.
Below is a link to a study on bifid T waves [link] pmc/articles/PMC2726157/ Study highlights: - they define bifid T waves as those that are "notched, being the 2 peaks separate from each other by a notch with duration greater than or equal to 0.02 There is a biphasic down-up T wave appearance in V1 and V2.
See here for management of Polymorphic Ventricular Tachycardia , which includes Torsades. However, this review references the Sterns article above, which by my reading does not state this. Literature Two Articles on Rapid Replacement of Potassium Efficacy and safety of potassium infusion therapy in hypokalemic critically ill patients.
As we've discussed on numerous other posts in Dr. Smith's ECG Blog ( See My Comment at the bottom of the page in the May 5, 2022 post) — a growing number of conditions other than Brugada Syndrome have been found to temporarily produce a Brugada-1 ECG pattern. Sinus Tachycardia ( common in any trauma patient. ).
Is it ventricular tachycardia (VT) due to hyperK or is it a supraventricular rhythm with hyperK? Here are other posts on hyperK, large calcium doses for hyperK, and ventricular tachycardia in hyperK Weakness, prolonged PR interval, wide complex, ventricular tachycardia Very Wide and Very Fast, What is it? How would you treat?
Here is the ECG: Sinus tachycardia. However, this review references the Sterns article above, which by my reading does not state this. This patient presented with severe DKA. What do you think? The computer and physician reader wrote: "ST depression, consider subendocardial injury." What else?
As we have described multiple times on this blog, false positive "pericarditis" kills by distracting the clinician from actual emergencies including OMI, dissection, PE, and others. The vast majority of cases with chest pain diffuse ST Elevation are due to Normal Variant ST Elevation, NOT to pericarditis. 15-9/6/2017 ).
4 Unfortunately, this article provides no electrocardiographic, echo, or angiographic data, so it is not certain that these high levels were in the absence of acute MI. NOTE: For those interested — I review in detail determination of the artifact “culprit extremity” in My Comment in the September 27, 2019 post of Dr. Smith’s ECG Blog.
See this articles: Heart Failure with Preserved Ejection Fraction (NEJM review) One etiology of LVH on the ECG is Hypertrophic Cardiolmyopathy (HOCM), and sometimes ECGs in patients with HOCM are specific for HOCM. LVH can have very thick-walled ventricles and a correspondingly small LV cavity.
At the bottom of the post, I have re-printed the section on aVR in my article on the ECG in ACS from the Canadian Journal of Cardiology: New Insights Into the Use of the 12-Lead Electrocardiogram for Diagnosing Acute Myocardial Infarction in the Emergency Department Case 1.
10 The 2014 ACC/AHA guidelines for the Management of Patients with Valvular Heart Disease , referencing this article, gives this recommendation: "CLASS IIb 1. Hypotension may of course be a result of a brady- or tachydysrhythmia. 2) Hypoxia, including poisons of oxidative phosphorylation such as HS, CO, CN.
Although the shock is no doubt partly a result of poor pump function, with low stroke volume, especially of the RV, it should be compensated for by tachycardia. Here is full text of this article. Cardiac output is stroke volume x rate, so this patient needs a higher heart rate. This is a perfect indication for atropine.
Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. An ECG was recorded: This shows a regular narrow complex tachycardia at a rate of about 160. See my quick review of atrial tachycardia below) The tachycardia spontaneously resolved. BP:143/99, Pulse 109, Temp 37.2 °C
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Annotated Bibliography For an excellent overview of ED Syncope management , see this article by Kessler C et al.
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. Her temperature was 106 degrees. As part of the workup, she underwent an ECG.
Smith comments : Wide complex tachycardia. The differential diagnosis of WCT is: 1) Sinus tachycardia with "aberrancy" (in this case RBBB and LAFB), but there are no P-waves and the QRS morphology is not typical of simple RBBB/LAFB. Also, if the rate is constant, not wavering up and down, it is highly unlikely to be sinus tachycardia.
In my review of the literature, there are many articles which purport to demonstrate an acutely increased risk of plaque rupture from emotional stress, but I could not find any credible case reports that were not at least as likely to be takotsubo.
We showed this in this article in JAMA Cardiology. 2025.110515 [link] Abstract Objective: The administration of amiodarone or lidocaine is recommended during the resuscitation of out-of-hospital cardiac arrest (OHCA) patients presenting with defibrillation-refractory or recurrent ventricular fibrillation or ventricular tachycardia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content