This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
As reviewed in ECG Blog #350 — t he clinical significance of Wellens' Syndrome — is that its recognition tells you that the patient has a high-grade LAD narrowing with presumably "hot" thrombus h avin g high propensity to propagate and/or totally occlude the LAD at any point in time ( including immediately ). What is W ellens’ S yndrome ?
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
Meyers, Weingart and Smith published their OMI Manifesto — in which they extensively document the critically important concept that management of acute MI by separation into a “STEMI” vs “non-STEMI” classification is an irreversibly flawed approach.
See these 2 articles Association between pre-hospital chest pain severity and myocardial injury in ST elevation myocardial infarction: A post-hoc analysis of the AVOID study Author links open overlay panel [link] 1 Background We sought to determine if an association exists between prehospital chest pain severity and markers of myocardial injury.
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. See these posts: Chest Pain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab?
This is obviously unreliable data, as Dr. Smith’s Blog has published 51 cases of OMI with ECGs labeled ‘normal’ , 35 of which were identified by the Queen of Hearts – with 10 examples here. Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.
See my formula for differentiating anterior LV aneurysm (that is to say, persistent ST elevation after old MI) from acute anterior STEMI. See this full text link to an article from JAMA on PCI in patients who present at 12 to 48 hours. Here is a link to a blog post with the formula , which we have recently validated and will publish.
Subtle as a STEMI." (i.e., HYPERACUTE T-WAVES ARE EASILY RECOGNIZED BY THE QUEEN OF HEARTS HYPERACUTE T-WAVES DO NOT EVOLVE INTO ST ELEVATION -- THIS IS A MYTH Pendell and I are about to submit an article on ECG findings in total 100% LAD Occlusion (LAD OMI). None of the 20 ever evolved to STEMI criteria.
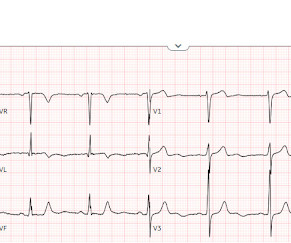
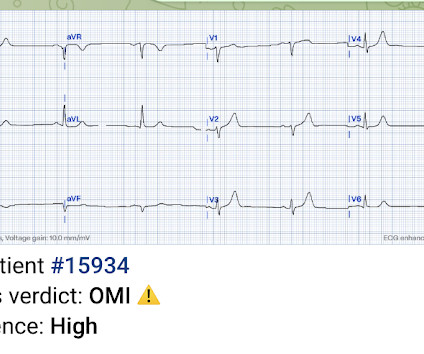
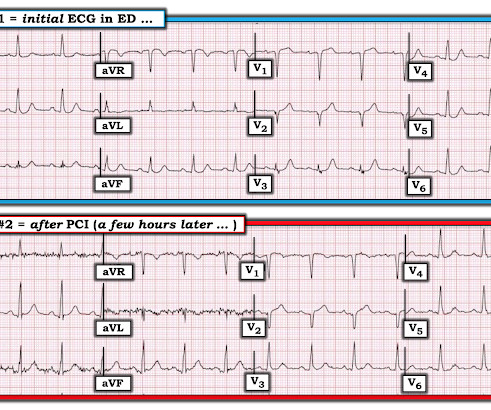
This was a machine read STEMI positive OMI. Readers of this blog can easily appreciate the hyperacute T waves in the precordium, clearest in V1-V4. The meaning of this quote is that at times, something as obvious as the dramatic anterior lead ST elevation that we see in today's tracing is not the result of an acute LAD STEMI.
Many systems now refrain from showing computer "normal" ECGs to the busy emergency physicians at triage because of very poorly conceived articles that say that if the computer algorithm says "normal," the emergency physician should not be bothered. We have shown many examples of this on this blog. No further follow up is available.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? This is the response he got: Interventionist: "No STEMI, no cath. After stabilizing the patient and recording more ECGs, he tried again: Interventionalist: "It isn't a STEMI." It is a STEMI equivalent. And the article was rejected.
The cath lab was activated, as it should be with transient STEMI. See this case of transient STEMI: Spontaneous Reperfusion and Re-occlusion - My Bad Thinking Contributes to a Death. Computer algorithms are completely unreliable at diagnosing STEMI, with both poor sensitivity and poor specificity.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. baseline (this is what most recommend but seems like far too much QRS widening to me) = See these articles and this graphic: 1. The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chest pain.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. The LAD has reperfused early. This was recorded 2.5
The Non-STEMI, which was an OMI, was diagnosed much faster with AI on the ECG than with troponin. I described "Posterior Reperfusion T-waves" in this article. For more on ECG findings in pulmonary disease — Check out My Comment in the May 31, 2024 post in Dr. Smith's ECG Blog ). It had never been described before.
Non-randomized trials show better outcomes (neurologic survival) using this device; see this article in Resuscitation: Head and Thorax Elevation during cardiopulmonary resuscitation using circulatory adjuncts is associated with improved survival. The patient had ROSC and maintained it. First — Some thoughts on the post -resuscitation ECG.
Quiz : What percent of full blown STEMI have an open artery with normal flow at angiogram? It too is "normal" and you decide that this is not OMI or STEMI and you just decide to get troponins. I would expect TIMI-3 flow (normal flow, no persistent ischemia) with a culprit in the RCA (or possibly Circumflex). Jesse McLaren et al.
Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4. Finally, Transient STEMI should be taken emergently to the cath lab. Normalization of Diagnostic For STEMI Prehospital ECG with Nitroglycerin Therapy. If the initial ECG was diagnostic for STEMI the paramedic called to mobilize the reperfusion team.
Here, I do not see OMI (although the ECG is falsely STEMI positive with just over 1 mm STE in V1 and about 2.5 In the 500+ Comments I have written on Dr. Smith's ECG Blog since becoming an Associate Editor in 2018 — I do not believe we have had a case of RA-LL lead reversal. What do you think? mm STE in V2).
I have posted previous such cases, but in searching my own blog, I could not find them. Dr. Smith also referenced an article by Knotts et al, showing that even when diffuse subendocardial ischemia is due to coronary disease — that only a minority of patients had severe LMain coronary disease as the cause. Is this OMI?
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." In the Marchik article, (assuming they defined it the same way, and the methods do not specify this), S1Q3T3 was found in 8.5% What is an S1Q3T3? Very few studies define S1Q3T3. Kosuge et al.
He has a great blog too: ECG Interpretation He is also well known on the Facebook EKG Club page , where you can learn tons about ECGs: Here is his response, with the first ECG labelled: Hello Steve & Avinash. Is there STEMI? It is commonly seen in the reperfusion setting. AIVR is NOT common in otherwise healthy children.
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 Here is another classic article. This T-wave inversion morphology is very specific for Wellens' waves.
This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI." He was worried for inferior MI and ordered another, which was recorded 15 minutes later: Now clearly and obviously diagnostic of inferior STEMI. Unknown algorithm Interpretation: Inferior ST elevation, with reciprocal ST depression in aVL.
They do not study whether this wave differentiates between MI and non-MI, between STEMI and NonSTEMI, or between OMI and NOMI. Here is an ECG with N-waves, from the article: Are these N-waves in our ECG? Another ECG was recorded: Obvious inferior, posterior, lateral STEMI What is the infarct artery? This is hard to tell.
In a recent article (J Electrocardiol this year, see reference below), peak trop onin I levels in takotsubo presenting with ST Elevation were median 1.02 Note 2: This article fails to specify whether it was troponin I or T, but I contacted the institution and they used exclusively troponin I during that time period. From Gue at al.
Smith and Meyers to diagnose both obvious (STEMI) and subtle OMI. We've previously discussed the all-too-often ignored entity known as MINOCA ( = MI with N on- O bstructive C oronary A rteries ) — which we detailed in the November 30, 2022 post in Dr. Smith's ECG Blog ( See My Comment at the bottom of the page ). It was trained by Drs.
Without seeing the patient, my interpretation of the first ECG was: likely normal variant ST-elevation (early repolarization), with a small possibility of pericarditis, and almost no possibility of acute coronary occlusion (STEMI). and therefore highly unlikely to be STEMI. in V6 and J-point notching.
This was just published in JAMA Internal Medicine: The de Winter Electrocardiogram Pattern Evolving From Hyperacute T Waves It reminded me that many believe, due to the assertions in the original de Winter's article, that de Winter's waves are stable. Interventionalist at the Receiving Hospital: "No STEMI, no cath. They are too narrow!
Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiac arrest with unrecognized STEMI, died. Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAH) on the admission ECG.
If it is maximal in V1-V4, and the patient's presentation in consistent with ACS (as this certainly is), then it is DIAGNOSTIC of Occlusion with 90% specificity (We have an upcoming article that proves this). Because we are hypnotized the STEMI paradigm. "If If there is no STEMI, there is no emergent problem and the patient can wait."
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
See these posts for Wellens' mimics: Pseudo-Wellens' Syndrome due to Left Ventricular Hypertrophy (LVH) Anterior STEMI? It even meets STEMI criteria: 2.5 Is it Wellens' Syndrome? This was the first ECG (ECG #1) recorded during pain : This shows ST elevation and hyperacute T-waves in the LAD distribution.
This meets "STEMI criteria" However, there is very high voltage, with a very deep S-wave in V2 and tall R-wave in V4. The morphology is not right for STEMI. My interpretation: LVH with secondary ST-T abnormalities, exaggerated by stress, not a STEMI. This is very good evidence that the ST elevation is not due to STEMI.
Could this be Septal STEMI (STE in V1 and aVR, with reciprocal ST depression in V4-V6?), Aslanger added in the limitations in his article: " Theoretically, an isolated basal inferoseptal infarction or an acute inferior MI in the presence of previous infarctions that may change the orientation of lesion vector can also cause a similar picture.
This is a troponin I level that is almost exclusively seen in STEMI. So this is either a case of MINOCA, or a case of Type II STEMI. If the arrest had another etiology (such as old scar), and the ST elevation is due to severe shock, then it is a type II STEMI. I believe the latter (type II STEMI) is most likely.
Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI. But what we truly care about is coronary occlusion, for which STEMI is just a surrogate that is only about 75% sensitive for occlusion. Some are STEMI-equivalents.
3) STEMI criteria failed to identify this acute coronary occlusion, like many others. Normal QRS-T angle From this article: Ziegler R and Bloomfield DK. Yes, there are valuable articles from 50 years ago! 2) Contemporary troponins only start to rise 4-6 hours after the onset of acute coronary occlusion.
These findings are very subtle but suspicious for LAD occlusion, as we have seen in many similar (but less difficult) cases on this blog: A man in his sixties with chest pain at midnight with undetectable troponin How long would you like to wait for your Occlusion MI to show a STEMI? Learning Points: Not all OMI will present as STEMIs.
Here is an article I wrote: Updates on the ECG in ACS. The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present.
4 Unfortunately, this article provides no electrocardiographic, echo, or angiographic data, so it is not certain that these high levels were in the absence of acute MI. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease.
There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI). In fact, the STE is widespread, mimicking an anterior STEMI. Here is full text of this article.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content