This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
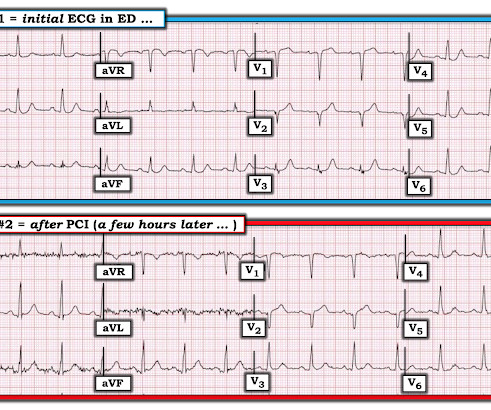
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
Written by Jesse McLaren A healthy 75 year old developed 7/10 chestpain associated with diaphoresis and nausea, which began on exertion but persisted. Below is the first ECG recorded by paramedics after 2 hours of chestpain, interpreted by the machine as “possible inferior ischemia”. What do you think?
Written by Jesse McLaren Three patients presented with acute chestpain and ECGs that were labeled by the computer as completely normal, and which was confirmed by the final cardiology interpretation (which is blinded to patient outcome) also as completely normal. What do you think? It should never have been published.
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. See these posts: ChestPain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab? What do you think?
I had a previous case of an adolescent with trauma and chestpain who also had AIVR: An adolescent with trauma, chestpain, and a wide complex rhythm From this blog post: "AIVR is NOT common in otherwise healthy children.
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. PEARL: Most patients who present with new chestpain + ECG changes + positive troponin — will not need Cardiac MRI. This was sent to me by a partner: "Curious what you think of this one we had overnight.
An elderly woman presented with chestpain that radiated to the back for several hours. The first troponin returned at 0.099 ng/mL (elevated, consistent with Non-Occlusion MI) Providers were concerned with aortic dissection, so they order a chest aorta CT. It is essentially normal.
A 60 year old with chestpain presented to the ED. In the December 5, 2022 post of Dr. Smith's ECG Blog — We show 4 additional cases of this pulse-tap artifact. Here is his first ECG: What do you think? It looks bizarre, doesn't it? There are lots of ST-T abnormalities, but they just don't look recognizable.
There was apparently no syncope and he had no bony injuries, but he did complain of left sided chestpain. His chest was tender. A bedside cardiac ultrasound was normal. An ECG was recorded: Avinash was understandably confused by this ECG. He wrote: "ECG 1 - shows wide ???IVCD IVCD type rhythm ??
Written and submitted by Ashley Mogul, with edits by Pendell Meyers and Steve Smith A man in his 40s with recent smoking cessation but otherwise no known past medical history presented due to chestpain since the previous evening. The pain has been constant and associated with vomiting and diaphoresis.
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. Case A 40-something male presented to triage. There are classic Wellens' waves in V2-V5.
In the Marchik article, (assuming they defined it the same way, and the methods do not specify this), among patients with suspicion for PE, S1Q3T3 was found in 8.5% While I still had questions about this case given the limited information provided ( ie, Was chestpain in this younger adult diabetic from acute PE?
Written by Pendell Meyers, edits by Smith and Grauer A man in his late 20s with history of asthma presented to the ED with a transient episode of chestpain and shortness of breath after finishing a 4-mile run. His symptoms of chestpain and shortness of breath were attributed to an asthma exacerbation during exercise.
Sent by anonymous A man in his 40s with no previous heart disease presented within 30 minutes of onset of acute chestpain that started while exercising. We have shown many examples of this on this blog. Three patients with chestpain and “normal” ECGs: which had OMI? Chestpain and a computer ‘normal’ ECG.
After only 90 minutes of chestpain, the first troponin was unsurprisingly in the normal range at 11ng/L (normal <26 in males and <16 in females), so the emergency physician waited for repeat troponin. Chestpain still persists. Paged cardiology 0800: patient complains of chestpain. Cardiology aware.
In the hope of dispelling continued dependence on millimeter-based STEMI criteria — we’ve published numerous cases in recent years in Dr. Smith’s ECG Blog of acute OMI ( O cclusion-based M yocardial I nfarction ) , in which patients have benefited from acute reperfusion despite not satisfying “STEMI criteria”.
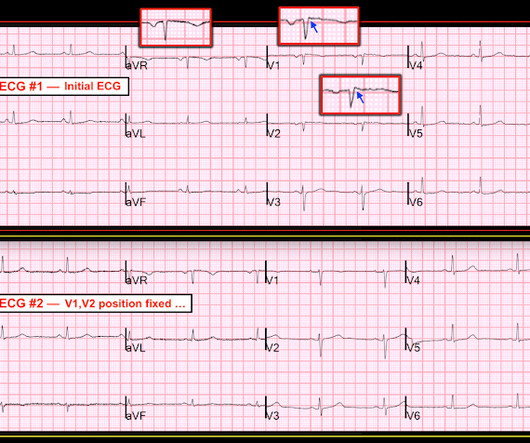
A middle-aged woman presented with chestpain. Brooks Walsh ( [link] ) has a great article on this topic, though he does not discuss septal Q-waves as a result: Misplacing V1 and V2 can have clinical consequences (full text). 27, 2018 blog post ). She had no history of cardiac disease.
A 60-something awoke with 10/10 crushing chestpain. But the patient's chestpain continues and so you order a 2nd ECG (ECG 2 here). It also is interpreted as "normal" and the patient's chestpain is now 10/10 and so you are really diligent and order a 3rd ECG. He walked in to triage. Jesse McLaren et al.
Non-randomized trials show better outcomes (neurologic survival) using this device; see this article in Resuscitation: Head and Thorax Elevation during cardiopulmonary resuscitation using circulatory adjuncts is associated with improved survival. The patient had ROSC and maintained it. First — Some thoughts on the post -resuscitation ECG.
This patient had the onset of chestpain 24 hours before arrival to the ED. I described "Posterior Reperfusion T-waves" in this article. For more on ECG findings in pulmonary disease — Check out My Comment in the May 31, 2024 post in Dr. Smith's ECG Blog ). Here is that ECG: Original ECG What do you think?
On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. As I illustrated in detail in My Comment of the October 3, 2018 post of Dr. Smith's ECG Blog — I favor a qualitative approach based on shape. The question is, does she need to go urgently to the cath lab or can she wait.
Written by Willy Frick A 50 year old man with no medical history presented with acute onset substernal chestpain. Readers of this blog can easily appreciate the hyperacute T waves in the precordium, clearest in V1-V4. His ECG is shown below. Pretty obvious anterior current of injury. This was a machine read STEMI positive OMI.
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chestpain. EMS gave 324 mg aspirin and 3 sublingual NTG, which the patient stated reduced the substernal chestpain from an 8/10 to 4/10. I have posted previous such cases, but in searching my own blog, I could not find them.
While fully acknowledging that "Sometimes ya gotta be there!" — in order to optimally assess the patient — the clinical definition of hemodynamic stability is for the patient to be without significant symptoms such as chestpain, shortness of breath, hypotension and/or mental status changes — as a direct result of the fast heart rate.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chestpain. Several hours prior to presentation, while driving his truck, he started experiencing new central chestpain, without radiation, aggravating/alleviating factors, or other associated symptoms.
The supposition that beta blockade in the presence of cocaine intoxication would lead to unopposed alpha constriction is not based in accurate pharmacology, and the study that showed this effect with human intracoronary administration was done, as mentioned in the article, with propranolol, a nonselective beta blocker. Marcus, G. Flores, E.D.
There was no chestpain or SOB at the tim of the ECG: Computerized QTc is 464 ms A previous ECG from 8 years prior was normal. Absence of chestpain or SOB at the time of the ECG is important; had the patient had active chestpain, I would have recommended at least an emergency formal echo, if not cath lab activation.
The patient had come to the ED for SOB, but without any chestpain. Other cases of Pulse Tapping Artifact: Acute chestpain and a bizarre ECG Bizarre (Hyperacute??) NOTE: I reproduce in the ADDENDUM below ( in Figures-3 , - 4 and - 5 ) — the 3-page article by Rowlands and Moore ( J. He had a 10 pound weight loss.
She did not report any chestpain or pressure. She was brought to the Emergency Department and this ECG was recorded while she was still feeling nauseous but denied chestpain, shortness of breath, or other symptoms: What do you think? A male in his 60s with chestpain A Male in his 60s with Chestpain.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. Jernberg T, et al.
This case was recently posted by Tyron Maartens on Facebook EKG club (he agreed to let me post it here), with the following clinical information: "42 year old male with two weeks of intermittent chest discomfort, awoke 4 hours prior to this ECG with a more severe, heavy chestpain (5/10). BP 112/80, SpO2 100%.
This was just published in JAMA Internal Medicine: The de Winter Electrocardiogram Pattern Evolving From Hyperacute T Waves It reminded me that many believe, due to the assertions in the original de Winter's article, that de Winter's waves are stable. He was a 30-something with chestpain. Here is one case of a patient I saw.
She went on to describe her chestpain as a "buffalo sitting on my chest" and a "weird" sensation in her jaw for 1 hour prior to arrival, associated with lightheadedness and diaphoresis. The patient was given fentanyl initially for chestpain with minimal effect and then vomited which was followed by zofran and famotidine.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
He said that his pain does not feel like his previous episode of pericarditis, and is not related to meals. He denied chestpain, shortness of breath, nausea, fever, chills, rashes, cough, and leg pain. He admitted to lifting some heavy objects a few days ago but denied trauma. in V6 and J-point notching.
This was sent by : Jacob Smith, DO Emergency Medicine Resident Ohio Health Doctors Hospital Emergency Residency Christopher Lloyd, DO, FACEP Director of Clinical Education, USACS Midwest Case A 30 year old patient presents to triage with chestpain. link] Here is the history: A 30 yo man presented complaining of severe chestpain.
This 42 yo diabetic male presented with cough and foot pain. In spite of aggressive questioning, he denied chestpain, but he did tell one triage nurse that he had had some chest burning, and so he underwent an ECG: There are deep Q-waves and QS-waves in precordial leads V2-V3, with a bit of R-wave left in V4.
The patient's chestpain had resolved by the time of the ECG 2. But it does prove that the patient has coronary disease and makes the probability that his chestpain is due to ACS very very high. He presents with an episode of brief, new-onset chestpain that had resolved by the time E CG # 1 was obtained.
Wellens' is a syndrome of a painless period following an anginal (chestpain) event. Chestpain, SOB, Precordial T-wave inversions, and positive troponin. She also complained of generalized weakness, lightheadedness, diaphoresis, chestpain, and cough. What is the Diagnosis? What is an S1Q3T3? Kosuge et al.
And some similar ECGs from Pulmonary Embolism: A young woman with altered mental status and hypotension An elderly woman transferred to you for chestpain, shortness of breath, and positive troponin - does she need the cath lab now? S1Q3T3, or even just the T3, may help to differentiate Wellens' from PE. What is an S1Q3T3?
Post by Smith, with short article by Angie Lobo ( [link] ), a third year intermal medicine resident at Abbott Northwestern Hospital Case A 30-something woman with no past history, who is very fit and athletic, presented with 1.5 hours of substernal chest pressure. She had zero CAD risk factors. Circulation, 137(19), p.e523.
Acute chestpain and a bizarre ECG Bizarre (Hyperacute??) Arterial pulse tapping artifact [link] This online article references the article below by Emre Aslanger, a great guy who occasionally corresponds with me about ECGs. Figure-3: Page 475 from the Rowlands and Moore article that I reference above.
This 50-something otherwise healthy male presented with one hour of epigastric and lower chestpain. Here is an ECG with N-waves, from the article: Are these N-waves in our ECG? Here is his initial ECG: What do you think? The QRS is 90 ms and the QTc is 400 ms. There is also ST depression in V2 and V3.
Case A 39-year-old male without prior medical history presents with chestpain that started 2 hours prior to presentation. He says that the pain intensity was 10/10 at home but now about 4/10. Despite the clinical stability and decreasing pain, this patient needs an immediate angiogram. Here are his publications.)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content