This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The most-popular HEART SISTERS posts from 2023 were all over the map - from 'Struggle Care' to sweating, hanging up that iconic Red Dress, or cardiacarrest on the toilet!
Here is an article I wrote: Updates on the ECG in ACS. Cardiacarrest can cause diffuse subendocardial ischemia, usually transient (it often resolves as time goes by after ROSC). STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? If you want to understand aVR, read this.]
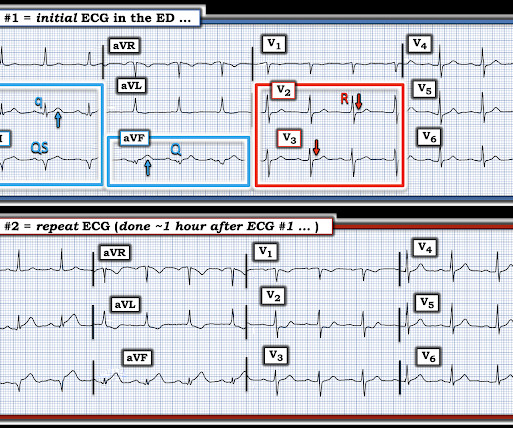
About 45 minutes after the second EKG, the patient was found in cardiacarrest. Later the next day, she went into cardiacarrest again. By the time I saw the repeat EKG, the patient was already in cardiacarrest. For more on Precordial Swirl — See the October 15, 2022 post in Dr. Smith's ECG Blog ).
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. The patient had ROSC and maintained it.
4 Unfortunately, this article provides no electrocardiographic, echo, or angiographic data, so it is not certain that these high levels were in the absence of acute MI. NOTE: For those interested — I review in detail determination of the artifact “culprit extremity” in My Comment in the September 27, 2019 post of Dr. Smith’s ECG Blog.
baseline (this is what most recommend but seems like far too much QRS widening to me) = See these articles and this graphic: 1. As we've often emphasized on Dr. Smith's ECG Blog — it is rare in practice to see LMCA occlusion, because most such patients die before reaching the hospital.
Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiacarrest with unrecognized STEMI, died. Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAH) on the admission ECG.
NOTE: The ECGs in today's case are recorded in the Cabrera Format ( See Dr. Grauer Comment in the October 26, 2020 post of Dr. Smith's ECG Blog for review on the Cabrera Format ). Regarding AFib with WPW: The very rapid heart rate and at times extremely short R-R intervals put the patient with AFib and WPW at risk of cardiacarrest from VFib.
Day 5 this was recorded: Still a hint of Brugada in V1 One month later: Normalized When the patient awoke, he and his family reported a family history of close relatives with cardiacarrest of uncertain etiology. The patient himself had never had syncope or dysrhythmias. It is free full text.
If cardiacarrest from hypokalemia is imminent (i.e., However, this review references the Sterns article above, which by my reading does not state this. As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 mEq/L for every 100 mEq total body deficit. mEq/L, from 1.9
If cardiacarrest from hypokalemia is imminent (i.e., CASE : Prehospital CardiacArrest due to Hypokalemia I recently had a case of prehospital cardiacarrest that turned out to be due to hypokalemia. As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2
I suspect this is Type 2 MI due to prolonged severe hypotension from cardiacarrest. Shark Fin morphology has been discussed a number of times on Dr. Smith’s ECG Blog ( For review — See the June 11, 2018 post and the January 24, 2020 post , to name just 2 instances ). A list of conditions that can cause this is below.
Steve, what do you think of this ECG in this CardiacArrest Patient?" A woman in her 50s with dyspnea and bradycardia A patient with cardiacarrest, ROSC, and right bundle branch block (RBBB). HyperKalemia with CardiacArrest. Is this just right bundle branch block? 72; Issue 9; 2018.
If cardiacarrest from hypokalemia is imminent (i.e., However, this review references the Sterns article above, which by my reading does not state this. As I indicated above, in our cardiacarrest case, after pushing 40 mEq, the K only went up to 4.2 How would you treat? mEq/L for every 100 mEq total body deficit.
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. In a recent article (J Electrocardiol this year, see reference below), peak trop onin I levels in takotsubo presenting with ST Elevation were median 1.02 She was defibrillated and resuscitated. ng/mL [IQR: 0.46, 2.35].
This article discusses correction of the QT interval for rate. I've been working on this a long time, thought about submitting it to a journal, but decided it gets more readers on this blog. The article is written by Dr. Smith and Dr. Friedman. In that article, they do not say what is a dangerously short QT is (e.g.
And the article was rejected. This blog is full of cases in which OMI that did not meet STEMI millimeter criteria were dismissed. IF they don’t — they will continue to overlook obvious OMIs that deserve to undergo prompt cardiac catheterization for optimal care.
As we've discussed on numerous other posts in Dr. Smith's ECG Blog ( See My Comment at the bottom of the page in the May 5, 2022 post) — a growing number of conditions other than Brugada Syndrome have been found to temporarily produce a Brugada-1 ECG pattern. What are the ECG Findings of Cardiac Contusion?
The article is edited by Smith. In addition to a spontaneous or induced Brugada-1 ECG pattern, criteria for B rugada S yndrome require one or more of the following: History of cardiacarrest, of polymorphoic VT, or of non-vagal syncope — positive family history of sudden death at an early age — a similar ECG in close relatives.
He had a previous MI with cardiacarrest 2 years prior. Down below are 3 more cases and a discussion of how to differentiate false positive isolated STE in aVL from True positive. Case A 47 year old male called 911 for severe chest pain. He was clammy and looked unwell. Is this due to coronary occlusion? Some are STEMI-equivalents.
Aslanger added in the limitations in his article: " Theoretically, an isolated basal inferoseptal infarction or an acute inferior MI in the presence of previous infarctions that may change the orientation of lesion vector can also cause a similar picture. (Our with ADDED STE in III?
If a patient presents with chest pain and a normal heart rate, or with shockable cardiacarrest, then ischemic appearing ST elevation is STEMI until proven otherwise. An excellent review of myocardial bridging, with full text: [link] Myocardial bridging is when the coronary artery, usually the LAD, dives into the myocardium.
Further history later: This patient personally has no further high risk features (syncope / presyncope), but her mother had sudden cardiacarrest in sleep. We repeated the ECG: Brugada pattern is mostly resolved. Follow up the next AM: Brugada pattern is resolved Below is what the electrophysiologist recommended. 8, 2019 ) — ( Jan.
You can read the abstract (o r of course the entire article) at the link provided. We are lucky this patient did not have a cardiacarrest while in the Waiting Room. Here is the PMcardio Queen of Hearts interpretation of the ECG: STEMI equivalent detected. Inferior and posterior OMI without STEMI criteria. Very interesting.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content