This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
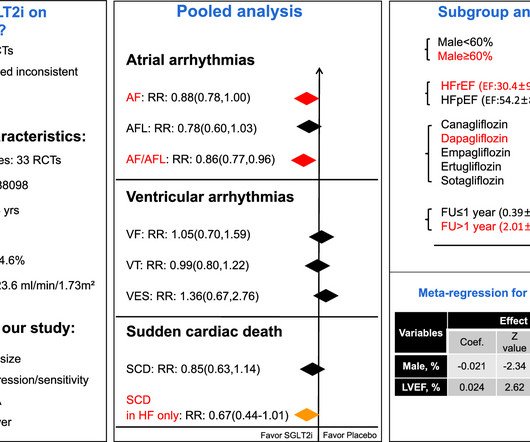
Objective We aimed to assess the effect of SGLT2i on arrhythmias by conducting a meta-analysis using data from randomized controlled trials(RCTs). Background Sodium-glucose co-transporter 2 inhibitors (SGLT2i) have shown cardioprotective effects via multiple mechanisms that may also contribute to decrease arrhythmias risk.
Sympathetic nervous system hyperactivity plays a major role in the pathogenesis of ventricular arrhythmias following myocardial infarction (MI).1,2 1,2 The stellate ganglia are an important nexus point for sympathetic innervation to the heart.3
Background Ventricular arrhythmias (VAs) frequently occur in the acute phase of myocarditis. Possible arrhythmic recurrences and the risk of suddencardiacdeath (SCD) in this setting are reasons for concern, and limited data have been published to guide clinical management of these patients. to 0.53, p=0.13).
He developed cardiac arrest shortly after the ECG in Figure-1 was recorded. What is the most likely cause of this arrhythmia? IMPRESSION: Given the presence of a wide tachycardia — with 2 distinct QRS morphologies, and no sign of P waves — a presumed diagnosis of B i D irectional Ventricular Tachycardia has to be made.
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. The granulomatous inflammation affects the heart, causing an infiltrative cardiomyopathy The most common manifestations of cardiac sarcoidosis are atrioventricular (AV) block and ventricular tachyarrhythmias (VT).
Brugada syndrome (BrS) is a primary arrhythmia syndrome associated with suddencardiacdeath.1 1 Pathogenic/likely pathogenic (P/LP) SCN5A variants are found in about 20%25% of patients and are associated with a higher burden of ventricular arrhythmias (VAs).2
Recent advancements in catheter ablation for structural ventricular tachycardia (VT), such as high-density mapping and cardiac imaging-based detection of target areas, have significantly improved the efficacy of ablation procedures.
Catecholaminergic polymorphic ventricular tachycardia (CPVT) has been identified as a notable cause of suddencardiacdeath in children and young adults.1 Catecholaminergic polymorphic ventricular tachycardia (CPVT) has been identified as a notable cause of suddencardiacdeath in children and young adults.1
For the past four decades, implantable cardioverter defibrillator (ICD) therapy has become the standard of care for preventing suddencardiacdeath in high-risk individuals. The rate of ICD implantation has risen due to the increasing population age and the growing prevalence of cardiacarrhythmias.
Patients with Brugada syndrome who are asymptomatic and have no ventricular tachycardia/ventricular fibrillation inducibility by programmed electrical stimulation are at extremely low risk of experiencing late life-threatening arrhythmias. Methods Patients with BrS ( n = 523; mean age, 51 ± 13 years; male, n = 497) were enrolled.
Suddencardiacdeath remains the main killer of adults in industrialized countries and reentrant ventricular arrhythmia (VA) is its main underlying mechanism1.
Cardiovascular mortality, driven by suddencardiacdeath, is the main reason for dying while waiting for heart transplantation (HTx). Aims Timely referrals for transplantation and left ventricular assist device (LVAD) play a key role in favourable outcomes in patients with advanced heart failure (HF).
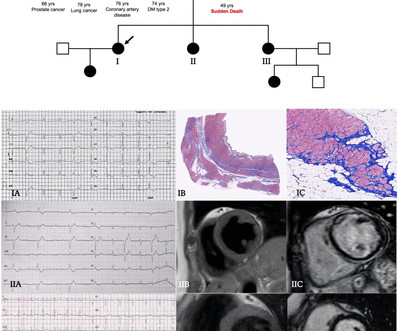
Clinical contexts leading to diagnosis were SCD in 3 (6%), ventricular arrhythmias in 15 (29%), chest pain in 8 (15%), heart failure in 6 (12%) and familial screening in 20 (38%). Significant right ventricular involvement was an exclusion criterion. Results Fifty-two patients (63% males, age 45 years (31–53)) composed the study cohort.
A few decades ago all suddencardiac arrests with documented ventricular fibrillation (VF) and structurally normal hearts were diagnosed as idiopathic ventricular fibrillation (IVF).
There are a number of things to look for in an ECG that can hint at arrhythmia as the cause of an apparent seizure. There is a run of polymorphic ventricular tachycardia — which given the QT prolongation, qualifies as Torsades de Points ( TdP ). Below are some of the conditions to be aware of: Preexcitation Brugada syndrome.
It can automatically detect life threatening ventricular arrhythmias and treat them, either with a shock or, sometimes by overdrive pacing. You may be knowing that one of the causes for inappropriate ICD shocks, is supraventricular arrhythmia, wrongly detected by the defibrillator as a ventricular arrhythmia and giving a shock.
ICDs are safe and effective for terminating life-threatening ventricular arrhythmias; transvenous leads, which run through the veins and into the heart, can result in complications. It works by briefly delivering pacing pulses to the heart at a rate faster than the tachycardia.
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a disease characterised by fibrofatty replacement of the ventricular myocardium due to specific mutations, leading to ventricular arrhythmias and suddencardiacdeath. channels, Connexin 43 and Wnt signalling, potentially modifying myocardial fibrosis.
Chagas disease (ChD) was associated with increased rates of ventricular tachycardia and ventricular fibrillation in ICD patients only in the initial two periods, but there was no statistical difference in the last period. Time periods were chosen based on the establishment of the Arrhythmia Service in 2011.
Brugada syndrome is thought to account for about one fourth of suddencardiacdeaths in individuals with structurally normal heart. This is the proposed mechanism of precipitation of arrhythmias in Brugada syndrome during febrile episodes. I am always happy to see this ECG of Brugada syndrome as it was sent to me by Prof.
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7]. per year. There was a 0.9%
See this even more interesting and more dramatic and fascinating case: History of Hypertrophic Cardiomyopathy (HOCM), with Tachycardia and High Lactate = My Comment by K EN G RAUER, MD ( 10/28 /2023 ): = QUESTION: For clarity in Figure-1 — I've reproduced today's ECG without the long lead rhythm strip. If so — WHO to screen?
Suddencardiacdeath in cardiomyoptahies: incidence, risk factors and prevention. ABSTRACT Cardiomyopathies are a significant contributor to cardiovascular morbidity and mortality, mainly due to the development of heart failure and increased risk of suddencardiacdeath (SCD).
Methods and ResultsWe retrospectively analyzed 401 patients with cardiac sarcoidosis without sustained ventricular arrhythmia at diagnosis. The primary end point was an FVAE, defined as the combined endpoint of documented ventricular tachycardia or ventricular fibrillation and suddencardiacdeath.
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. Her temperature was 106 degrees. As part of the workup, she underwent an ECG.
ABSTRACT Background Mitral annular disjunction (MAD) carries an increased risk of complex ventricular arrhythmias, which can lead to suddencardiacdeath. Many of these patients undergo implantable cardioverter defibrillator (ICD) implantation, but their ICD outcomes are not known.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content