This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Note the Timed Contents that I detail below facilitate finding specific material. == ECG Podcast #4 — All About Comparison ECGs for 12-Leads and Arrhythmias ( Comparing ECGs seems so "easy" to do — but so often is not done correctly! ) — published by Mayo Clinic CV Podcast Series on 5/21/2024 ( 35 minutes ). What are the problems?
Cardiac arrest #3: ST depression, Is it STEMI? Confirmation of sinus tachycardia should be easy to verify when the heart rate slows a little bit ( as the patient's condition improves ) — allowing clearer definition between the T and P waves. In this case, the cath lab was activated and the patient had a normal angiogram.
It's a very "fun" ECG, with initial ectopic atrial tachycardia (negative P waves in inferior leads conducting 1:1 with the QRSs), followed by spontaneous resolution to sinus rhythm. In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. Triage ECG: What do you think?
22:25 — What if you have a regular SVT ( = narrow-complex tachycardia ) without obvious P waves? ( And regarding arrhythmias: For more on the regular WCT — See My Comment in the May 5, 2020 post and in the April 15, 2020 post in Dr. Smith's ECG Blog. 11:35 — My views on: Will the computer ever be able to interpret complex arrhythmias?
His previous echo one month prior shows the same thing: “consistent with old infarct in LAD vascular territory, with EF 45%” "I think there is something else causing his tachycardia which is exaggerating his EKG findings and mimicking an acute myocardial infarction." The patient spontaneously converted back to sinus tachycardia.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Additionally, his cardiac telemetry monitor showed runs of accelerated idioventricular rhythm, a benign arrhythmia often associated with coronary reperfusion. It was stented.
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. Notice there is tachycardia. So there was 3-vessel disease, but with an acute posterior STEMI.
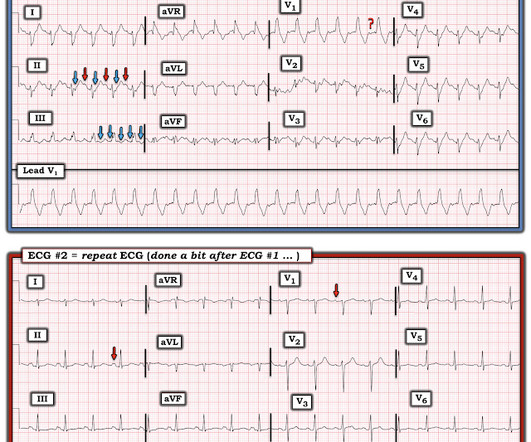
First, we have a narrow-complex, regular tachycardia, with a rate of about 135-140. This narrows our differential for the rhythm down to sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT, or SVT), and atrial flutter. Is this inferor STEMI? Tachycardia and ST Elevation. Christmas Eve Special Gift!!
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
The finding of a fairly regular, wide tachycardia without clear sign of atrial activity ( especially when seen in an acutely symptomatic patient ) — should immediately prompt a diagnosis of VT until proven otherwise. The rhythm looks fairly regular — and atrial activity is absent. What is S hark F in M orphology ?
There is sinus tachycardia. Sinus tachycardia, which exaggerates ST segments and implies that there is another pathology. I have always said that tachycardia should argue against acute MI unless there is cardiogenic shock or 2 simultaneous pathologies. Here is that ECG: What do you think? See Table for diagnostic utility.
Idioventricular rhythm is a common "reperfusion arrhythmia." In other words, after reperfusion therapy for STEMI, the appearance of AIVR is usually a good sign, meaning that the artery is reperfused. In fact, there may be less than 1 mm of concordant ST depression in lead V3. But it is not conclusive. 3) AV nodal re-entry????
During active chest pain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF. A "STEMI alert" was called and soon cancelled. Shortly after receiving epinephrine, the patient developed new leg cramps and chest pain. Pain lasted for approximately 45 minutes.
Here, I do not see OMI (although the ECG is falsely STEMI positive with just over 1 mm STE in V1 and about 2.5 This is sinus tachycardia (rhythm) with complete heart block (AV node function) with ventricular escape rate just below 30. Never forget that sinus tachycardia is the scariest arrhythmia. What do you think?
Here is the ECG: Sinus tachycardia. Discussion See this post: STEMI with Life-Threatening Hypokalemia and Incessant Torsades de Pointes I could find very little literature on the treatment of severe life-threatening hypokalemia. malignant ventricular arrhythmias are present), rapid replacement of potassium is required.
Is it ventricular tachycardia (VT) due to hyperK or is it a supraventricular rhythm with hyperK? Here are other posts on hyperK, large calcium doses for hyperK, and ventricular tachycardia in hyperK Weakness, prolonged PR interval, wide complex, ventricular tachycardia Very Wide and Very Fast, What is it? How would you treat?
The finding of all negative QRS complexes in leads V3-thru- V6 therefore strongly suggests that the arrhythmia-associated impulse is not traveling over an AP ( Steurer et al — Clin. Given the rapid rate of the tachycardia and the amorphous shape of the QRS — the decision was made to sedate the patient and cardiovert.
No arrhythmias occurred en route. C linically — the rhythm we see in the long lead II of ECG #3 behaves similar to MAT, even though there is no tachycardia. The case was discussed with the cardiology fellow at the nearest tertiary care center and arrangements were made to fly the patient via HEMS.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. myocardial infarction), arrhythmias, valvular pathology, shunts, or outflow obstructions. What do you see?
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished.
There are three mechanisms of arrhythmia: automatic, re-entry, and triggered. The most common triggered arrhythmia is Torsades de Pointes. Automatic activity refers to enhanced pacemaking function (typically from a non sinus node source), for example atrial tachycardia. Is there STEMI? What is the rhythm? Moffat, M.
MY Initial Thoughts: In my experience — all-too-many emergency providers fail to appreciate the potential contribution that a brief ( 1-to-2 line ) history may convey when interpreting arrhythmias. when the usual negative P wave deflection of sinus tachycardia is nowhere to be found in lead V1 )? What do YOU think?
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. However, he suddenly developed a series of malignant ventricular arrhythmias. This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). What do you think?
ECG is consistent with severe hypokalemia and/or hypomagnesemia causing prolonged QT (QU) at high risk of Torsades (which is polymorphic ventricular tachycardia in the setting of a long QT interval). Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management Cardiac Arrest. Is it STEMI?
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. 2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. A rectal temperature was obtained which read 107.9 Bicarb 20, Lactate 4.2,
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. Her temperature was 106 degrees. As part of the workup, she underwent an ECG.
PEARL # 3: Knowing there is an acute inferior STEMI I looked next to see if there is also acute posterior involvement ( which so often accompanies inferior MI ). But larger-than-expected Q waves in each of the inferior leads ( especially in lead III ) are probably the result of this patients ongoing acute inferior STEMI.
The paramedics diagnosis was "Possible Anterolateral STEMI." More proof that a huge STEMI may have normal or near normal initial troponin. If breakthrough ventricular arrhythmias occurred, additional 50-mg boluses were given every 5 minutes, as needed to a maximum of 325 mg. The final angiographic result is very good.
ECG met STEMI criteria and was labeled STEMI by computer interpretation. While traditionally described as “benign early repolarization”, they have been associated with J wave syndromes along with Brugada syndrome, causing ventricular arrhythmias (1, 2). Take home : Not all STEs are STEMIs or OMIs. What do you think?
Final Diagnosis: "STEMI" (of course, as you can see in the ECGs above, this is not true, by definition this was NSTEMI. But the "final diagnosis" commonly just reflects whether the patient was given emergent therapy or not, regardless of the definition of STEMI/NSTEMI). In other words, millimeters really don't matter!
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content